
Dognosis: Unleashing Canine Superpowers
How an interspecies team in Bangalore is conjuring nature's most ancient magic to slay the Emperor of All Maladies


Hey folks👋
Welcome to the 846 new Tigerfeathers Dogfeathers subscribers who’ve joined the pack since our last essay.
As you will have gathered, today’s piece will be littered with an irresponsible number of canine-themed puns. So if that’s the kind of thing you like and you’ve not subscribed yet, we suggest you paws and fix that👇🐾
This edition of Tigerfeathers is presented by…Mumbai Tech Week

The authors of this newsletter have been accused of many things. Perhaps at the top of that list: being unabashed Bombayphiles (and guilty as charged🤷♂️). So it shouldn’t surprise anyone that we’ve had a soft spot for Mumbai Tech Week since its first edition. It’s hard not to root for a festival that’s essentially a two-day argument that this city belongs in the same conversation as any tech hub on the planet.
MTW is now in its third edition. Like the past two iterations, this one is hosted by TEAM - the Tech Entrepreneurs Association of Mumbai - which, since launching in 2022, has been hustling to bring together the city’s disparate founders, developers, investors, policymakers and service providers into a single spirited community.
The 2026 edition of Mumbai Tech Week runs from 29–30 May at the Jio World Convention Centre, with satellite events dotted across the city from 25–28 May. This year’s theme is ‘AI in Action’, and the programming has been curated to reflect it. That means less panel debates and more live showcases from practitioners. The people you’ll hear from this year aren’t analysts or futurists, but operators and founders actually deploying this stuff at scale, across some of India's most recognisable companies.
You can have a look at the agenda using the link below. And if you’re keen to attend this year, TEAM is offering Tigerfeathers readers a 30% discount on your ticket price (valid till 10th May). Just use the code TIGERFEATHERS30 while checking out:
Also, if it moves the needle for you (in either direction), both the Tigerfeathers and Runtime crews will be hanging out at MTW. Let us know if you plan to be around or in town. We’d love to say hi.

Last October, the Dognosis office - a lush two-acre former pomegranate farm on the fringes of Bangalore - came to a brief but dignified standstill.
Two of their star personnel, who’d spent the morning diligently screening medical samples for the presence of life-threatening diseases, had been caught in what can only be described as a sordid act of mutual investigation just outside the testing room. Specifically, they were sniffing each other's butts.
To be clear, and to pre-empt any accusations of crassness, that wasn't a joke, and this was no joking matter. At Dognosis, it is simply a Tuesday. As are other not-entirely-kosher workplace behaviours, like the occasional theft of a colleague's lunch, the spontaneous nap in the middle of a working session, and an incident last monsoon that involved one team member ingesting what was, at the time, a fairly important sample. None of this is metaphor. These are real incidents. The HR policy is a work in progress, made considerably more complicated when half your ‘resources’ aren’t humans at all.
As an outsider, it would be entirely reasonable to question why any serious company would put up with employees that exhibit such…questionable norms around personal space and personal hygiene. There are two main responses to that line of inquiry:
One, they’re kinda cute.

And two, this four-legged team has evolved to do something that their two-legged counterparts could never do. To put it plainly, they are able to detect the presence of multiple cancers in your breath - requiring nothing more than a face mask and ten minutes of your time - at an accuracy that no machine on Earth has managed, without the need for a blood draw, a scan, or a hospital visit. And the only thing they ask for in exchange for providing this vital service, is a generous supply of treats, belly rubs, sunset walks through the hills of Nelamangala, and plenty of time in the newly installed company doggy pool.
It’s a pretty sweet deal, all things considered.
As you can tell, it isn’t hard to find the joke when it comes to Dognosis. But there is nothing funny about the ambitions of the company, the work they do everyday, and the progress they’ve made in the three years since planting their flag paws in Bommasandra (Bangalore), to build what they believe will become the world's most powerful early detection system for cancer.

Dognosis was founded in 2023 by Akash Kulgod and Itamar Bitan on a deceptively simple premise: that evolution had already solved a problem that modern medicine has been chasing for decades. Even amidst the advancing apparatus of modern diagnostics - liquid biopsies, full-body MRIs, genomic sequencers - we had yet to forge a cancer screening tool sensitive enough to catch cancer early, reliably, and cheaply enough to matter at scale. What the two founders of Dognosis realised - one building on his Honours thesis at Berkeley, the other counting on his decade-long experience as a Special Ops K9 trainer in Israel - was that the solution had been living in our homes the whole time.
The dog's nose - the product of fifteen millennia of co-evolution with humans - can detect the faint chemical whisper of cancer in your breath at a resolution that our machines, our algorithms, and our laboratory tests have never come close to. We have known since at least 2004 - when the first peer-reviewed studies came out of the UK - that trained dogs could detect cancer from breath and urine with startling accuracy. We have also consistently failed to do anything meaningful with that knowledge. The problem was that we had no way to standardise, scale, or scientifically validate what they were doing in a way that medicine could trust and deploy. The missing piece was never the dog, it was the interface between what the dog’s nose knows and what medicine can act on.
That's what Dognosis is building - the translation layer that turns an ancient biological superpower into legitimate medical infrastructure.
I first visited the Dognosis HQ last August, to scratch my own curiosity on a startup that’s gotten accustomed to raised eyebrows and skeptical looks from visitors, and also to making believers out of anyone who walks through the gate of their farmhouse facility.



Spending a morning at the Dognosis facility tends to have that effect on people. For starters, you get to hang out with an awesome group of dogs (and dog lovers). You get to see their process in motion and the infrastructure they’ve built - it’s like a canine amusement park where their doggie crew gets rewarded with treats for pointing out when a surgical face mask has a weird smell coming from it. You arrive with many questions. You leave with a different understanding of what's possible for both science and nature, a greater appreciation for man’s best friend, and a strong desire to tell someone about it.
At Tigerfeathers, we've developed something of a nose for these out-of-distribution ideas - companies that sit so far outside the normal frame of reference that most people either dismiss them immediately or can't stop thinking about them. For us, Dognosis sits firmly in the second category, and we’ve been itching (and scratching) to go deeper into their story for almost a year. In fact, we’d already hosted Akash for an extended conversation, waiting for the right moment to drop this…
…which brings us to today, and to the first Monday edition of this newsletter, prompted by a piece of news from Friday that’s been several months in the making:
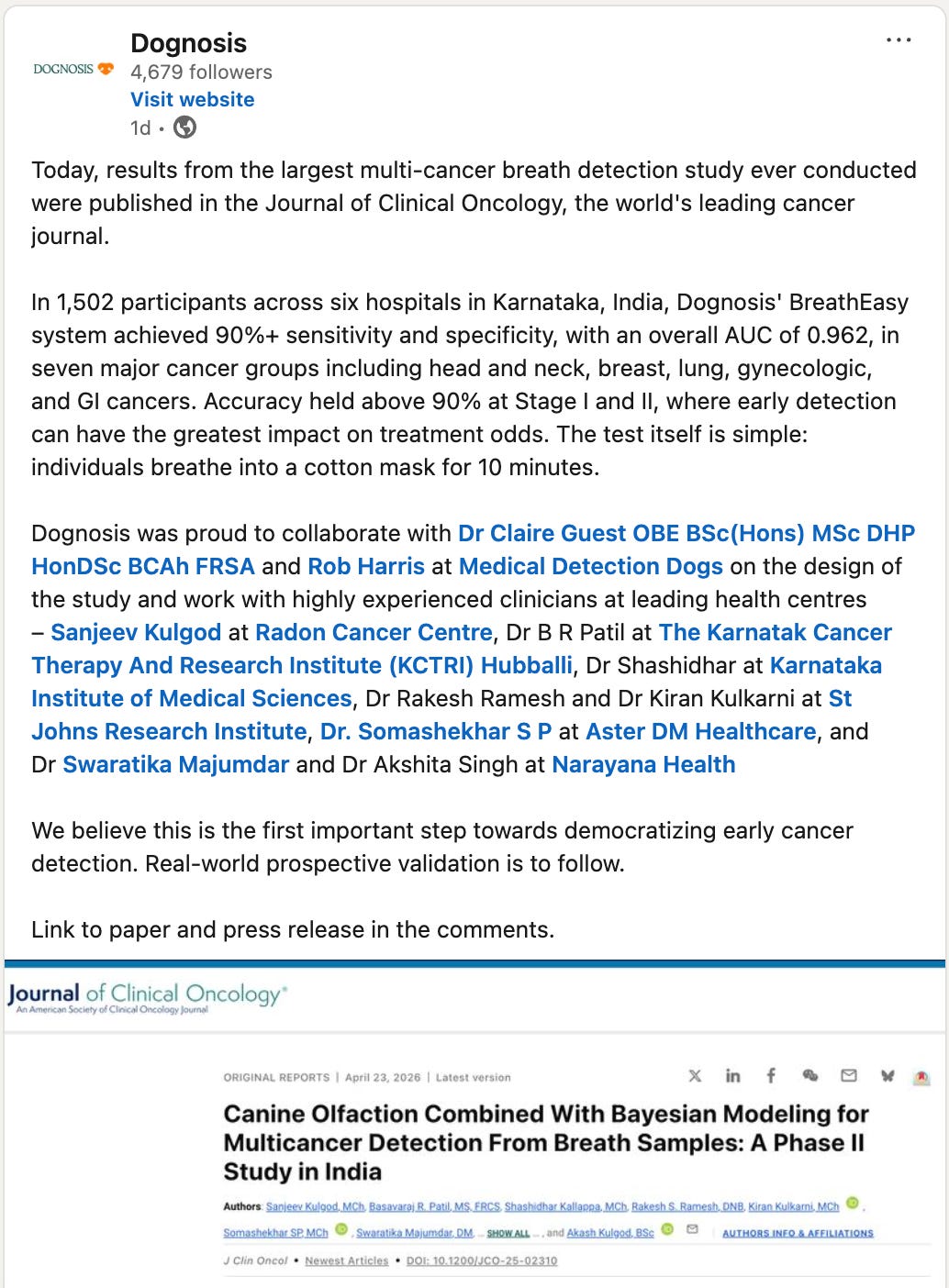
On Friday, the Journal of Clinical Oncology (JCO) - the world's leading cancer journal, the one that shapes how oncologists think and treat - published the results of Dognosis’ landmark Phase-2 study that was completed last year. It was the largest breath-based multi-cancer detection study ever conducted anywhere in the world. What they were trying to prove was that a team of trained dogs, equipped with sensors and AI, could reliably detect the presence of cancer in a breath sample, at early stage, across multiple cancer types, in a real-world clinical setting that looks nothing like a controlled laboratory. The results, to put it mildly, proved that they could.
When something appears in the JCO with a commissioned editorial, it does more than simply validate a finding. It tends to move it from the fringes into the mainstream conversation. So while the Dognosis team will be the first to admit that there’s a long way to go before this technology is ready for prime time, that there are still important milestones to cross before we can get to widespread clinical use - from our perspective, if the world’s most influential cancer journal thinks it’s time that people paid attention to the work being done in a former pomegranate farm in the outskirts of Bangalore, who are we to argue otherwise?
So to unpack the Dognosis story, Akash joined us for a long-form interview where he:
recounted the Dognosis journey right from conception to the recent JCO publication
talked about the history, the science, the technology and the commercial application of their core idea
painted a picture of his view of the future of medicine, and Dognosis’ role in it
offered a honest take on what is still unproven; what is next in their roadmap; and what their detractors get right
offered an even more honest take on the process of fundraising for such a novel idea (which recently and successfully ended with a seed round led by Accel Atoms)
and answered every question that I had (and suspect you have) about what it's actually like to be a dog at Dognosis.; where they come from and what their routines are; and why there should be a greater reverence for their abilities, and their role as humanity’s longtime protectors
It’s a long piece (of course), but should you make it to the end and think you might fancy a crack working at the frontier of healthcare and cancer care (and adorable canine care) in India, Dognosis is hiring across the board. If you’re a dog reading this and you think you might enjoy living in a big yard with lots of friends where you get treats for playing a sniffing game for 30 minutes everyday, then woof woof woof woof woof woof woof woof woof woof woof woof woof too.
Anyway, from where we’re sitting, Dognosis is an n-of-1 Indian startup with an n-of-1 story. We’re excited to have Akash here to tell it. Let’s get to it.

“As man lifts his eyes to the stars and meets the other inhabitants of this planet, his horizons become widened, his science deeper, his philosophy more in tune with the universe as it exists.”
- John Lilly, Communication Between Man & Dolphin
I. Origins
I know that you grew up in a family of doctors - your grandfather started one of the first hospitals in your hometown, your father is a gastroenterologist, your uncle is a doctor, your mother is a doctor, your older brother is a radiologist. What was growing up inside that world actually like?
I grew up in Belagavi, a mid-sized city in northern Karnataka that most people outside the state have never heard of. My dad's family is from a small hamlet nearby called Kulgod, which is also where I draw my last name. My first name, Akash, means something like ‘an ethereal fluid pervading the cosmos’ in Sanskrit. So normatively speaking, I was always going to end up doing something a little unhinged. My dad has a line he likes to quote, that “you need two things in life, strong wings and deep roots”. The roots, in our case, were very much Belagavi. And in our family, those roots ran straight into medicine.
To give you some perspective on your question, when I was growing up, at one point, we had eleven doctors and eleven dogs in the family simultaneously. We could have fielded a full cricket team of both.

By the way, I’ve used that joke so often it’s basically a dog-eared joke at this point. But it’s also quite real - medicine has been a formative part of my childhood. When you grow up with basically all your family members being doctors, talking about healthcare at the dinner table everyday, and spending time at their clinics in the evenings after school because they were working late, medicine kind of becomes the substrate of your childhood, like it did for mine.
That upbringing had two major consequences for me. One, it made me decide not to want to be a doctor. My half-joking reason for that is that because I realised all the medical departments were already covered by someone in the family. The more grounded reason was because I could see that no matter how hard my father and grandfather and my mother and uncles and aunts worked, there were only twenty-four hours in a day. As a doctor you don’t really have leverage on your time. You can only do so much as the hours you have, and the technology at your disposal allows you. It’s why I always say that there’s no ‘supply chain’ issue when it comes to tackling disease in India - it’s just a time issue.
The second consequence, was that it made me appreciate how profound medicine actually is. It’s hard to think of something more amazing than helping someone go from having a debilitating illness to being healthy. What is more radical than the transformation from sickness to health? All of the progress we expect for this current era of AI and technology, ultimately we want it to translate to giving people longer, healthier, happier lives. That’s the whole point of medicine, and it’s something I saw up close.

So those were the two things I took away from my upbringing - the realisation that medicine doesn’t really scale in the way I was looking for, and a deep appreciation for what it’s actually doing in the world.
Right, so help me plot the journey from childhood to Dognosis. You were equipped with these two realisations that came from your childhood. How did you find your way back into the world of healthcare and medicine?
Like I said, I knew then that I didn’t want to be a doctor. But I also wasn’t really the engineering type. If I had to really characterise myself at the time, the most accurate description would be a ‘reader’. I loved reading, and I read everything.
I read a lot of science fiction and also just regular science too - like Richard Dawkins was part of the childhood canon, along with Enid Blyton and Harry Potter. I was just fascinated by these big questions that only science could ask and answer. I decided to pursue scientific research too. At the time, there weren’t a lot of options in India for basic scientific research outside of medicine and engineering. And also, fun fact, I have an Irish passport, which made it more difficult and less straightforward for me to land a spot at IISc or ISER.

My best option was to go abroad, and I was lucky enough to get into the University of California, Berkeley, for my undergraduate degree, which turned out to be one of the best decisions of my life.
I read on your Substack that you took twenty-eight classes across fourteen departments, and worked in five different research labs at Berkeley. What were you actually looking for? What was the thread tying all of it together?
The beauty of a liberal arts degree is that you get to just dabble around a bit. It worked for me because I was interested in lots of things. I ended up majoring in cognitive science, which is cool because it’s like a central node that points to six other nodes that point to even more nodes and so on. You get to examine this question of how we can understand cognition through an interdisciplinary lens of neuroscience and AI and linguistics and philosophy and psychology. I liked it because it meant I could take a bunch of different classes.
I think for me the underlying thread through all of this study was a fascination with how intelligent, conscious beings try to make meaning. How do they represent the world? How do they understand each other?
I was particularly interested in this theme of ‘metaphor’, which seemed like an important piece of the puzzle - how humans across different languages use similar conceptual metaphors to make sense of abstract things.
Take the way we map space onto number, for instance. We don’t experience numbers directly, so we tend to picture them spatially - as points along a line. The number line correlates space with number in a very meaningful way. This mapping can differ across cultures, but the underlying instinct - to understand the abstract through the concrete - is strangely universal. And that applies not just to language, but to cognitive structures more broadly.
I was especially interested in this new theory of cognition and cognitive science called 4E cognition. 4E stands for embodied, enacted, embedded and extended. It was a theory being posited by researchers like Francisco Varela, who were fusing centuries-old ideas from Buddhist scholars with the kinds of things that modern cognitive scientists were finding in the lab and using scanners.
Essentially it suggests that the brain (and mind) isn’t the only place where cognition and meaning are being created. It’s actually in the body, in the way we interact with the environment, and in the tools we use. That was super interesting to think about because it’s the antithesis of the idea that our cognitive epicentres are just in the brain. It’s not ‘all just in your head’.

I was a lot more philosophical back then - now being a founder you're just way more pragmatic. But I still love this stuff. And there’s a connection there with Dognosis too. In a strange way it’s the scientific foundation of what we do today. Because what we’re saying is - yes, we’re going to try and measure what’s happening in the dog’s brain when it sniffs something. But the ‘meaning’ of the scent lies not just in the brain but in the dog’s behaviour and interactions with their environment too. But we’re probably getting ahead of ourselves…
Yes, natural follow up to that - how did dogs enter the picture at all?
Well, I was in my second or third year at Berkeley when the COVID pandemic hit. The world shut down. School went online, and I decided to take a gap semester. I moved back home to wait out the pandemic. This was in the summer of 2021, right in the midst of our terrible Second Wave. If you remember things had settled down a bit at the start of the year, it was looking like we might get back to normal, and suddenly we got hit with this second wave out of the blue.
My father was actually directing a hospital that was catering exclusively to COVID patients at the time. It had been a bold decision to set up the hospital that way because it had seemed like things had calmed down. People were like ‘okay, COVID’s gone, we don’t need to worry’. But he felt like there was a chance it could come back, and because he was one of the directors of the hospital, he thought it was important to plan accordingly.
And then that second wave hit and, well, things turned bad quickly. Even though they had done their best to prepare, he still had to make the kinds of difficult decisions that doctors around the world were being forced to make. Like who to admit to the hospital? Who not to admit? What should the calculus be to decide which people actually needed treatment versus the ones who might be okay?
I was seeing this all up close. And at that same time, it was all in the news. You were glued to the television and newspapers to get updates on what was happening around you. Around that time, I came across this article in the press that talked about how dogs were being deployed to detect COVID-19, it had something to do with the Indian Army. It did the rounds on social media too so a lot of people seemingly came across it as well.

There ended up being about a hundred organisations across all continents that were apparently trying some version of this - training dogs to sniff out COVID from the sweat or the presence of a person. And some of those results were genuinely staggering. There was one study, by a researcher named Hag-Ali, where the dogs turned out to be more accurate than the PCR gold standard that was being used to evaluate them. The yardstick itself was worse than the dogs.
When I came across this my first reaction was like, wait, what? Like, dogs can sniff out diseases?! Why wasn’t this something, I don’t know, they taught us in school or something?
I did some research and realised that it wasn’t just COVID. It was all kinds of diseases and it had been going on for a while. There were 20 years of peer reviewed publications suggesting dogs could sniff out diseases with really high accuracies from breath and urine and sweat. Cancer, diabetes, Parkinson's, they could apparently catch the scent of these diseases accurately and completely non-invasively.
The group in the UK that really pioneered this field - Medical Detection Dogs - had done the first study back in 2004. By the time I was reading about all of this, they held a Guinness World Record for the most diseases detected by a single dog group: twenty-eight. Twenty-eight diseases.

It blew my mind that, one, this was a thing and had been a thing. And two, the realisation that my love for dogs and my family’s love for dogs and this lineage of medicine had this amazing intersection that had been under our noses all this while, and I was somehow only now learning about it. And the third reaction was, wait a second, if the dogs can do this, then clearly they would have been super useful in Belgaum while my dad was making all these decisions. So where were all those dogs now? Where were all the disease sniffing dogs in general? This had to be more than just some cute press article, right? Those questions became lodged in my brain, and I could never shake the idea.
So did you end up going back to Berkeley?
Eventually the vaccine was developed, and the world began moving again. I went back for my final year to finish my degree, but I had this new purpose and new direction, so all my intellectual energy went towards understanding more about this field, and making these ideas more concrete.
I had a hunch that I could apply my cognitive science lens to this problem. I was lucky that I had taken classes on cognitive neuroscience, understanding how to employ these tools like fMRIs and BCIs to get more quantitative data on what was happening in the mind. I had classes on perception, and how it worked, and what sensory systems were doing as we moved through the world. The entirety of my college education was originally built on this substrate.
And then suddenly I was presented with this new problem statement, where you have this biological being - the dog - doing something that it turns out none of our machines could actually do, and we had no idea how they were doing it either.
It turns out people had tried to figure out what molecules the dogs were sniffing, but we couldn’t actually identify a consistent pattern. We had been trying to replicate what dogs had been doing with ‘electronic noses’, but had no luck with that either. In fact those experiments had all failed despite billions of dollars of investment and trials.
The conclusion really was that dogs seemed to be specially equipped to do this. We don’t know how. And the thing that was stopping humans from employing dogs to do this in a scalable way wasn’t any failings on the ability of dogs. It was that we didn’t know how to make sense of what the dogs were doing. It means we can’t really integrate that kind of capability into our medical system. That translation of the dogs’ ability for human comprehension seemed like the missing piece of the puzzle.
I remember you telling me when we first met that you actually did your final dissertation on canine olfaction. Walk me through what you actually figured out that year.
So at Berkeley you get to do an Honours thesis. You can choose anything you want to really dig into, find a couple of advisors, and write a dissertation around it. I obviously decided to lay the foundation for this canine olfaction business.
I basically looked for anyone who was doing anything related to canine olfaction or olfaction in general, or anything with dogs. It turns out there was a professor at Berkeley in the evolutionary neuroscience department who’d actually spent her career figuring out why and how olfaction and cognition had this very meaningful relationship.
In some sense, she was proposing that olfaction was the oldest sense. The very first living beings were detecting chemicals - that was the whole game, right? The E. coli bacteria is basically doing chemo-sensation - it's detecting chemical gradients in its environment, finding molecules of food by ‘smell’ in the most primitive sense of the word, and moving towards them. It's essentially the precursor to what we now call olfaction. And then all living beings and cognitive agents built on top of that.
And because smell was there first - because it was the original sense that living beings used to navigate and survive - it became woven into the deepest structures of the brain. So olfaction was kind of the scaffolding for things like intelligence and emotion and memory. And those connections never went away. Smell is the only sense that routes directly to the parts of the brain that govern emotion and memory - which is why Proust could write about the smell of Madeleine cakes transporting him to a completely different world in a way that a sound or a sight simply couldn't replicate.
So this professor had a very theoretical but also very rich background in this field - and as far as I could tell, she was the only person at Berkeley doing anything in this space. She also happened to have an ongoing project with search and rescue dogs, which made her the obvious person to approach. I cold emailed her. She didn't respond. So I just showed up to one of her classes and told her I wanted to do my thesis with her. She said yes
I then took a bunch of classes related to brain imaging methods and computational modelling, and started thinking through what it would actually take to build a practical solution to this problem. At the time the exercise was still fairly intellectual and academic in nature. But then I also took a small concrete step forward - a Berkeley entrepreneurship mini-grant allowed me to buy an open BCI system, which lets you build a basic EEG set-up from a chip board and a few electrodes. And I used it to collect some EEG data from a friend's dog. He's a chihuahua. His name is Woody.

Now, collecting EEG data from a Chihuahua is very difficult. And I quickly realised that, okay, you can try your best to tape an electrode to a tiny dog’s head, but, number one, the dog is just going to scratch it off. And number two, the data is kind of garbage. You don’t really get anything substantial.

It actually requires some serious engineering to figure out how to record electrical signals from a dog’s brain in a way that actually captures meaningful data. It wasn’t a simple problem. But it was cool to take that baby step, get some squiggly lines and be like, okay, like this is interesting.
For my final thesis, I fleshed out a framework for how you would actually do this - how you could build a rigorous, technically robust window into what a dog is smelling.
Can you elaborate on that? What does that actually mean?
So the title of my thesis was ‘Towards a 4E Approach to Canine Olfaction’. And 4E, like I said, means Embodied, Enacted, Embedded, Extended.
I argued that, okay, you can record from the dog’s brain while it’s sniffing things, but that’s actually not enough. You need to also know the dog’s embodied response - it’s respiratory responses, heart patterns, body language. You need to observe the whole path of how the dog acquired the meaning of the scent, because a scent does not have meaning independent of the process that gives it meaning. It's an active process.
What people may find interesting is that dogs might actually have an intuitive sense of the smell of cancer. This is actually a theory that’s out there because dogs are one of three animals to have a transmissible form of cancer. They have this kind of genitalia cancer that can move from dog to dog. And there’s a theory that that’s why dogs sniff each other’s butts to make sure the other dog is safe.

But more likely is the fact that most dogs don’t have an intuitive sense of cancer from the get-go. You have to shape the meaning of that i.e. of the scent of cancer, in a way that represents something to the dog.
My thesis talked about what that representation would look like, and how you might reverse engineer - or at least predict - what a dog is building when it learns the scent of a disease. It was theoretical, no actual experiments or data, but it helped establish an intellectual and scientific foundation that I felt was grounded in the best available science. And it pointed the way forward for how I could actually go about getting real data and building the thing.
What was the actual response to your thesis? What did your professor or the wider academic community think?
I don’t know if it ever got any real academic readership. An undergrad honours thesis is probably only read by the undergrad’s mother (I don’t know actually if my mother ever read my thesis either). But my thesis advisor really appreciated it. In fact, Berkeley grants about two undergraduate prizes for the Cognitive Science honours thesis every year - the Robert J. Glushko Prize for Distinguished Undergraduate Research - and mine was chosen as one of them.
My thesis advisor nominated it because she felt it was genuinely novel - that it added something real and useful to the field. She ended up writing a couple of papers building on the same ideas, taking them further into her own research on how olfaction and cognition are intertwined. In some sense, part of my thesis fed into her work. She was kind enough to acknowledge me in those papers, which was cool.
So that was the impact of the work. But it was also a turning point for me, because I was weighing up my options of, is the natural end for all of this canine olfaction stuff just a PhD? Or is it something else? While it was cool to write this paper and to think about where this could go academically, I wasn’t fully convinced about the academic path. I had my misgivings about how it seemed to be more about papers and publications. I felt like there was enough of that in this field. People have published plenty of studies about dogs sniffing out diseases. The thing that was missing was a real world application.
So you wrapped up things at Berkeley?
It was at the back of my mind that I needed to test this idea in the real world, so I planned to move back. Before that, I was lucky enough to be chosen as the commencement speaker for Berkeley Cognitive Science, which was a great honour. I think I gave a banger speech - at least that's what my friends said.
I was able to pay homage to the professors who’d shaped my time there. There's a Professor named David Presti, who teaches this legendary class called 'Drugs and the Brain', which had a big impact on me.
Sounds awesome. Was it a…practical class for you?

Let’s just say I was the co-president of the Psychedelic Science club at Berkeley. And in another life, I would have probably gone into psychedelic research. I was also involved with the Centre for the Study of Psychedelics that opened in Berkeley in 2021.
One lesson I learned there, which remains true, is that when it comes to something like depression - and so many other confounding mental health conditions - the psilocybin mushroom has been found to be way more effective than pretty much any pharmaceutical drug that has been conceived in the past sixty years of clinical trials. The mushroom has been around for millennia, and indigenous people around the world have known about the mushroom for millennia. It’s interesting, right, that nature has these solutions that already exist. We’ve relied on them for ages, and then almost forgotten about them. In some senses, modern medicine is playing catching up to what nature figured out long ago.
There’s an interesting parallel there with our work too, in that the dogs can do what our machines still cannot - that was part of my commencement speech. We've had this capability living in our homes for millennia. All we've been missing is the interface.
Anyway, right after giving that speech, I flew back to India the next day.
II. Scent of Home
Did you have a plan for what you were going to do in India?
Not really. I rushed back mainly to make it for my brother’s wedding, which was fun. I went from speech to revelry the next day.
But I was also in the minority in that I didn’t have a plan to stay back in the US. Almost everyone else from my batch from India stayed back. I just had this sense of wanting to come back to India. It wasn’t a very well defined reason except that I felt like I’d have the opportunity to do something bigger here.
I was still trying to figure out how to take this forward. A PhD didn’t feel like the right step, and it wasn’t a commercial venture then either. I was weighing up what to do next when I found out about this grant programme called Emergent Ventures (because I was a fan of the extended Tyler Cowen universe), and decided to give it a shot.
Three weeks after applying, I got on a call with Shruti Rajagopalan (who runs EV India) and ended up getting a grant from EV, which allowed me to have one year of open-ended exploration. It was a big enough grant to support me personally, along with the research and development that I wouldn’t have otherwise been able to do, like getting an EEG system and whatnot. That gave me the freedom and the belief in myself, and also the license to figure this out on my own without the need to be tied to a PhD or any other institution.
A few weeks later I got the chance to meet a bunch of other grantees at the Emergent Ventures Unconference that happened that year. That was almost as valuable as the grant itself. I met other young, ambitious people like Naman [Pushp], who were many years younger than me but already executing on these audacious ideas. They weren't waiting for anyone's permission or approval. I realised that there was nothing stopping me either.
So what did you do with the grant money?
I got on the road. I ended up becoming a visiting researcher at labs around the world that seemed to have found pieces of this puzzle. I emailed a bunch of professors everywhere to see if they would have me.
One of them was at the Tech4Animals Lab in the University of Haifa in Israel. She was doing work with computer vision and animal behaviour decoding. I just emailed her saying ‘Hey, I’m kind of working on this project. I would love to join you. You don’t need to pay me. You don’t even need to help me with a visa or anything. I’ll just show up. It would be great if we could work on something together’. She was pretty excited about the idea, and even helped me get an apartment in Haifa. So I went there to be a visiting researcher-slash-collaborator with her lab.
I did the same thing with a few other labs in Europe and the UK, where different parts of this research were happening. There’s a lab in Budapest - the Family Dog Project at ELTE University - that was doing cognitive neuroscience stuff with dogs, measuring canine EEG accurately in these experiments. And then there was this UK group, Medical Detection Dogs, that pioneered a lot of this work and had authored a lot of the groundbreaking studies.
And so for most of 2023, the year after graduating, I was just bouncing around learning from these different groups.
What did you learn from all of this exploration? Which pieces of the puzzle came together for you first?
I picked up something different at each lab. But I think the greater learning was that none of these labs had some secret sauce allowing them to do research that no one else could do. This was nothing specially ordained about their ability to solve these problems.
They had just gotten funding, hired people, and asked the right questions - which you could pursue from anywhere with the right tools. What also stuck out was that none of these labs had what I would have considered ‘state of the art’ equipment. What I mean by that is, no one had designed tools specifically for canine cognitive science. They were kind of adapting human tools to do the job.

My takeaway was that these labs were constrained by their academic orientation. They didn’t have devoted engineering teams working with them to design bespoke set ups. They were more focused on publishing papers.
Don’t get me wrong - I enjoyed working with those groups and learned a bunch. But the lesson that dawned on me was that doing a PhD wasn’t going to magically solve these problems. You needed an interdisciplinary team of engineers and scientists and canine professionals and dogs to actually make progress. You needed people that were unreasonably obsessed with solving this problem.
Is that the context of how you met your co-founder?
Yeah, sort of. When I was in Israel, I came across this guy - it was either through a mutual colleague or via LinkedIn - but I saw him doing a TV interview talking about disease detection dogs. He was apparently working at a startup called Prognose in Israel that was engaged in that type of thing. His name was Itamar Bitan. I reached out to him. We didn’t end up actually meeting when I was in Israel because he was flying out somewhere at the time, but it opened a channel of conversation.
I had eventually left Israel by the time he contacted me again. He reached out saying he had been reading my Substack, and that we should probably talk (side note to other founders, this is why you should write online). Anyway he reached out, we hopped on a call, it turned out the place he was travelling to was India. He called me from Himachal, and I remember he had this incredible mountain view.

I learned that he was Israeli, and he had served in Oketz. In Israel everyone serves in the military as a mandatory thing, and he was placed in Oketz - the IDF Special Operations K9 unit. In Oketz, you’re paired with a dog, and with that dog you do things like bomb detection, special operations. Each unit gets someone from Oketz. That person goes into a high-stress situation with their dog - the dog goes first, clears the way, and then all the other humans follow. They’re all trusting their lives on that dog’s nose.

After his service he became the first employee at Prognose. The founder of the company was the basically a dog wizard, like Israel’s like top dog trainer. They had been able to train dogs to detect breast cancer and Parkinson’s. Itamar had seen the dogs’ abilities firsthand, working with a team of labradors that could consistently identify the scent of disease on surgical masks from women who’d been diagnosed with breast cancer. The science was real. But he was leaving Prognose because things hadn’t worked out on the business end.
The founder’s original plan had been to sell detection tests online, via Facebook marketplace and things like that. But they hadn’t been able to figure out the regulatory challenges and go-to-market among other things. Itamar had been frustrated by this because he had seen firsthand that ‘yes, the dogs can clearly do this, and it’s solving a clear problem that exists’, but without a proper go-to-market strategy and well-defined product, these discoveries couldn’t really go anywhere.
He actually told me this story that I found fascinating - apparently at one point they had a brain cancer sample accidentally end up in a training set that had been designed only for breast cancer. The dogs still detected it. They hadn't been trained on brain cancer. They'd never sniffed it before. And they still found it. That moment crystallised something for Itamar: if the dogs could generalise across cancer types without ever being trained on them, it meant cancer had a common scent signature - something the dogs were uniquely capable of picking up. And if that was true, the right application wasn't training dogs to detect a single cancer. It was multi-cancer detection from the start.
As we talked, we also made another connection. Itamar said that the missing piece that would help with both go-to-market and product development was building some sort of technological apparatus that could understand what the dogs were thinking and doing - a scientific way to translate their behaviour into digital, quantifiable signatures, that you could train AI models on, which could potentially remove the need for a human in the loop. It was the same thesis that I had been developing myself, and his view was that this was the key that would unlock the ability to scale this idea.
I realised that Itamar was the perfect person to work with here. He had firsthand experience actually working with dogs, working alongside dogs, and training dogs to detect diseases. He’s probably trained more dogs on disease samples than anyone in the world. I didn’t know how to do any of this stuff. But beyond the skill-set fit - and I've thought about this a lot - what really mattered was the moment he committed. When someone else gets in and is all in, suddenly it's not just you and your self-doubt. It's two people. And that shift, emotionally, changes everything. I don't think people talk about this enough when they talk about co-founders. And yeah, after that first conversation I don’t think we ever stopped talking.
So after that first virtual conversation - how does that evolve to two strangers deciding to start up together?
At that time I was in Europe, in that other lab in Budapest. But the conversations started accelerating. We actually looped in my dad for a couple of these, because Itamar was curious about the landscape of Indian healthcare, of how things actually work here, how we could potentially go to market etc. In those conversations he was focused on trying to figure out what the business would actually look like, while I was trying to work out how any of this would even be possible.
Part of me thought that it was too early to broach the specifics of commercialisation. But I think what I grew to appreciate, and what I do now as well, is that he’s already seen this movie before. He wanted to take the next step. We both collectively realised that, for many reasons, India was the right place to do this - vast population, great talent, lower costs, greater opportunity to make an impact etc. It helped that he had fallen in love with the country after his time in Himachal too.
What we ended up doing was applying for a second Emergent Ventures grant in the summer of 2023. We got it, which allowed us to start planning for a small clinical trial, with the aim of building a set up to perform early stage cancer detection in India, using the team of dogs plus AI.
Was your dad a big help here? What did your family think of all this?
Well, my dad had come across these ideas the same time I did. He read about it in COVID. He found them intellectually fascinating. But like a lot of people digesting a piece of interesting news, it went in one ear and out the other.
 by Rebecca Yarros | Goodreads")
When he realised I was committed to studying this idea in depth, I think there was a small part of him that was worried about me, like ‘what is this kid doing with his life?’, especially as I was in the midst of wandering around the world. I think that sentiment persisted till even as recently as a year ago, where he wasn’t convinced this stuff was going anywhere.
But as things started falling into place, and it became clear that we had something that was both real and potentially impactful to the lives of so many people, he came around. Fast forward to the point where today he basically spends a solid two days every week as a senior medical advisor to Dognosis, helping with whatever needs helping out. He gives us grounding, because of his experience across all these different areas of healthcare, whether it’s things like interacting with patients, running our clinical operations, engaging with doctors, ensuring our entities are financially compliant, navigating the Indian bureaucracy - just imparting a lot of practical and specialised knowledge that neither me and Itamar have.
Things are even coming full circle now - my uncle Sanjeev Kulgod, who is a doctor in Hubballi, was actually the first author on our landmark JCO study. And my dad has gotten increasingly involved over the last six months, helping with our real-world pilots. It’s funny that, now when I talk to my dad, what was once a personal relationship is now a work relationship as well. It’s been nothing but awesome.
I always have to offer a big kudos to both him and my mom. They never criticised what I was doing. If anything they were just mildly worried what how I was choosing to spend my time. But they were always supportive, and they knew I was obsessed with this mission.
III. The Dogs
Okay maybe a good time to dive into the mission itself before we go ahead. If we rewind back - you talked about how nature has invented these solutions that machines have not gotten to yet. I know the mission statement of Dognosis is “unleashing canine superpowers”. So what is it about dogs? What has evolution bestowed on them that makes them olfactory problem solvers? What is it about them or their physiology that allows them to be exceptional at this?
It’s super interesting. I will caveat this by saying that humans don’t fully know the answer to this question yet. And also that this ability is perhaps not unique to dogs. A lot of animals have great olfactory sense-making systems, smell being the oldest sense and all.


It’s also still a kind of biological puzzle, where we’ve kind of figured out how vision and hearing work. But there are more questions than answers when it comes to how olfaction works.
My Berkeley thesis advisor had this line that I’ve never stopped thinking about - that ‘humans are blinded by vision’. As visually orientated cognitive agents, we just don’t naturally attend to the entire world of smell. We don’t have great language for it. We describe smells by referencing the thing that has the smell - it smells ‘like coffee’, ‘like a hospital’.

We can’t really describe smell parametrically the way we can with sound or colour. So we’ve also systematically underinvested in understanding olfaction. We’ve built cameras and microphones. We haven’t really built noses. And yet - and this is the striking bit - if you think about what AI has achieved in 2025: we now have systems with arguably human-comparable vision, hearing, and language. We have GPT-level reasoning. But the sense of smell remains almost entirely undigitised. The entire domain of olfactory intelligence is still terra incognita for AI. That’s extraordinary, given how ancient and fundamental the sense is.
Dogs specifically have a few things that allow them to do what they do in a way that humans can’t compete. They have way more olfactory receptors. There are more types of receptors, and more crammed into their nose in general. So they’re able to sense a whole bunch of different things. Their nose is itself sophisticated architecture. The lining of the mucus is such that the most soluble volatiles dissolve at the start and the less soluble ones dissolve further along. They’re literally running a kind of gas chromatography inside their nose, screening the molecules as they breathe in.

Then there are the slits on the side of the nose - you can see them if you look closely at a dog’s nose. Those allow the dog to create a vortex of air that wafts organic compounds toward the receptors in a way that optimises detection for diseases. Dogs can also breathe and sniff simultaneously, which we can’t.
But I think the most mind-bending thing is what’s happening in the brain, in their representation of these odours. Dogs seem unique in having a dedicated neural tract from the olfactory bulb directly to the occipital lobe (what is the visual cortex in humans). In us, that region is where visual processing happens and it dominates most of our cortex because we’re visual creatures. In dogs, the nose goes to that same region. They are quite literally seeing the world with their nose. The line between metaphor and biological reality gets very blurry there, because what does that even mean, right? We don’t know what the dog experiences the world like, but they’re seeing this world that is just represented in scent.
Maybe we can go back to your original discovery, of dogs being used to detect COVID, in many cases more reliably than the PCR tests everyone was using. What actually makes dogs good at disease detection? Obviously, they have a heightened sense of smell and much more sophisticated noses than us, beyond what we can even understand. But can you explain what’s happening when it comes to disease detection?
From reading your website, my simplistic understand of it is this: Your body constantly produces chemicals (that are detectable by scent) → When you have a disease (like cancer) those chemicals change → That change comes out in your breath → Because of their superior sense of smell, dogs can detect it. Is that basically right?
Pretty much. So let’s take a specific type of cancer to narrow this down, because ‘cancer’ in general is many different diseases. In the case of breast cancer, what we know based on what the dogs have ‘told’ us, and what we’ve been able to piece together, is that breast cancer will change the innate scent that a human gives out.
And the scent can be from breath or it can be from a medium like urine. Let’s take breath for now because it’s what we focus on, and it’s also the most interesting because breath has the richest scent when it comes to what a human is giving out (far more complex than other biofluids like blood or urine).
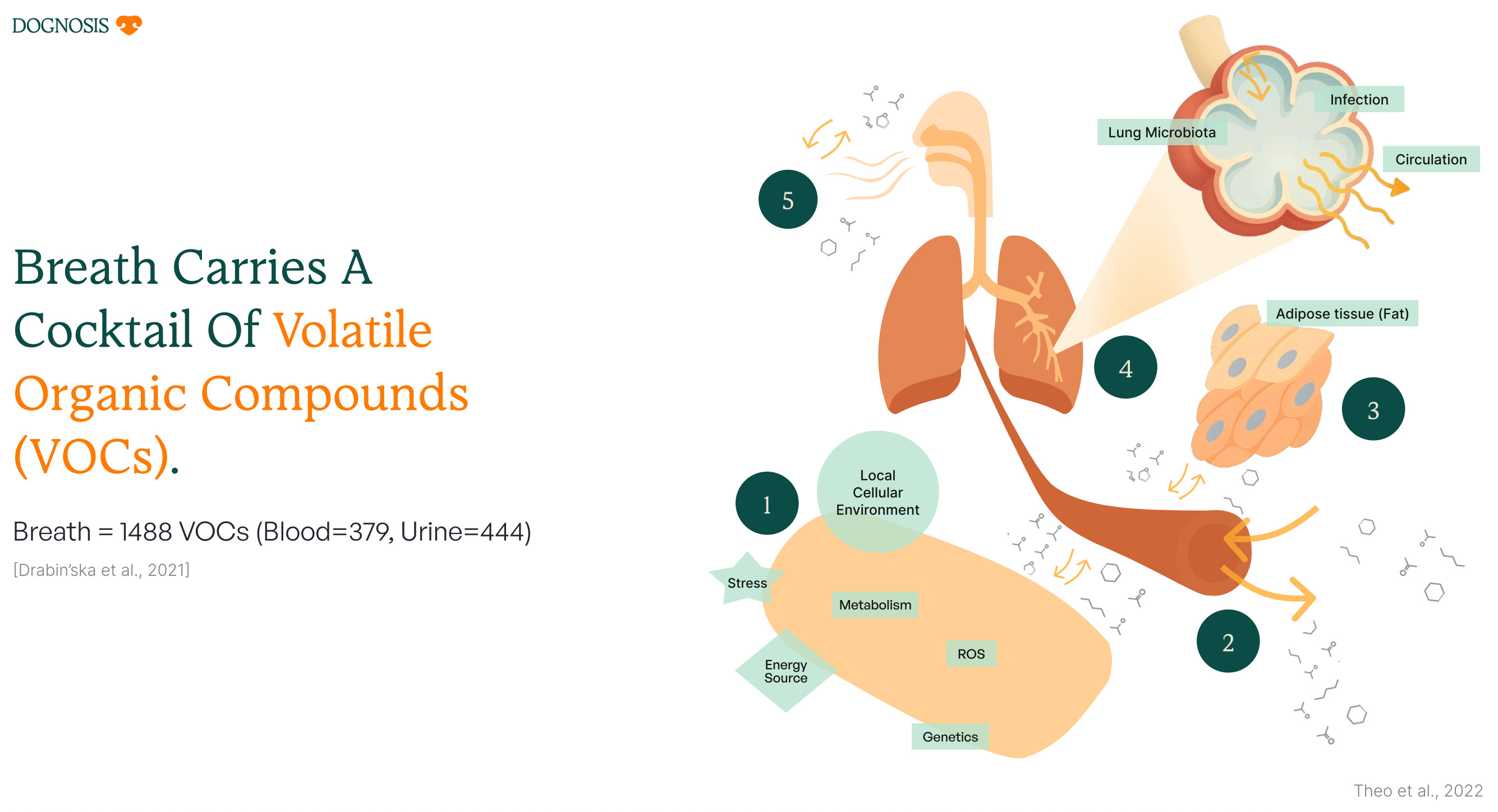
So scent is made up of VOCs - i.e. volatile organic compounds. It just means any molecule that is light enough to be sent out of the body via the breath. We know breath consists of around 1500 different VOCs that we’ve been able to catalogue. So at any point you will constantly be breathing out this cocktail of 1500 compounds - and that concentration and composition will also vary from person to person. But what we know is that if you have a disease like breast cancer or diabetes or any other infectious disease, that cocktail will change. And the remarkable thing is that cocktail changes in a way that is actually consistent across individuals. So we might all have different base cocktails, but a specific disease will give a specific flavour to that cocktail.
And with a sophisticated enough sensor, enough data, and a clever enough algorithm, you can decode that scent pattern and detect the disease - that’s what the dogs are good at. Essentially if you give them enough variations of this cocktail with that flavour, they can detect that flavour whenever they come across it again. The super interesting thing is that you would think this flavour is something we could identify with our machines - like okay, these twenty molecules, or this change in concentration, this is the master template for this disease. It turns out with something like cancer, we just can’t identify it that way, to that level of precision. We literally don’t know how. But we know the dogs are picking it up. So it must be real.
I think the best analogy here is, say you’re a coffee drinker. If I give you some coffee, and I blindfold you, and I ask, what is this? You can tell me it’s coffee. But if I ask you what molecules are in the scent of this coffee, you probably have no idea. I have no idea either.

But there are hundreds of molecules in the smell of coffee. It’s actually a pretty complex scent. We don’t know what those molecules are, but we can definitely identify it when we smell it. And that’s basically what the dogs are doing. They have this perceptual representation of the scent of a disease that isn't easily broken down into molecules and concentrations.
Can you help us understand why exactly we can’t just build a machine to do what the dog’s nose does? What’s stopping us? What’s different about how you’re approaching it?
People have been trying to do exactly this for decades and spent billions on it. Humans have tried to figure out what molecules the dogs were sniffing - and we’ve been unable to identify a consistent pattern. We tried to replicate what the dogs do with electronic noses - that failed despite the investment. And yet governments around the world still rely on dogs at borders, airports, and on the battlefield, because the skill is so valuable, even though our machines haven’t gotten there yet.

There are two main reasons why we can’t just replicate this.
The first is resolution. Dogs are detecting at parts per trillion. To give you a sense of what parts per trillion actually means: it's the equivalent of detecting a single drop of food colouring in twenty Olympic swimming pools. That's what the dog is doing with every breath it takes. Our most advanced analytical instruments (gas chromatography-mass spectrometry) work at parts per million. That’s a million-fold difference in sensitivity. At early-stage cancer, the signal in breath is extremely faint. You need that resolution. And that’s not an engineering gap you can just close by building a better machine. It’s the actual physical ceiling for those instruments. And while groups around the world have been trying to close that gap for decades, we still haven't come close to matching the dog's limit of detection
The second is deeper. It’s the sense-making itself. Olfaction is computationally different from vision or hearing in a way that’s easy to miss. With a picture you can describe it in terms of colour, frequency, spatial relationships. With a sound you can do frequencies and amplitudes. With smell you hit something much stranger - the perceptual experience isn’t a clean function of the molecules present.
There's a famous example in chemistry - sometimes called ‘Sell's triplets’ - that really illustrates this. You take two molecules that are nearly identical in chemical structure. You'd expect them to smell similar. But one of them smells like vanilla and the other like citrus. Completely different. Then you take two molecules that are structurally very different from each other - and they both smell floral. Almost indistinguishable. The mapping from molecular structure to perceptual experience is nonlinear, and we don't fully understand it. So even if you can detect which molecules are present - which itself is already incredibly hard - that doesn't tell you what the smell means.

What this means for cancer detection is striking. Scientists have spent decades trying to identify the specific molecules that signal cancer in breath. And when you look across all those studies, the picture is a mess - the same cancer shows up with completely different VOC profiles across different patients, and different diseases end up looking almost identical at the molecular level. The scent of cancer isn't encoded in a neat set of molecules you can put on a checklist. It's a holistic pattern - a gestalt - that the dog's brain somehow reads, even when our best instruments can't find it.
In our case it’s why we think the real solution runs in the opposite direction from what most people have tried. Rather than starting from molecules and trying to work up to percepts, you start with the percepts - with the dog’s own perceptual judgment - and work backwards. The dog is the oracle. It already knows what the scent of cancer means. What we’re doing is building the interface to read that judgment and learn from it. Think of it as the dog teaching the machine to smell, rather than the machine trying to replace the nose.
So what’s actually stopped us from using dogs’ abilities in a scalable way was never the dog’s nose. It was the human on the other end of the leash. We didn’t know how to read what the dog was doing in a way that was standardised, quantifiable, scalable. That’s the problem we’re actually solving.
I’m curious, when did humans actually discover this? Obviously we’ve been using dogs to detect explosives on the battlefield or drugs at airports, but when did we become cognisant of how impressive this ability is? Like, when did dogs become working professionals across all these different areas?
Well in some sense, dogs are the first other species that humans learnt to collaborate with, right? Man and dog is the prototype of interspecies alignment. Obviously it was wolves who first struck this deal, something like 15,000 years ago - we don’t know all the details.
But essentially it looked like this - the wolves were like ‘hey, we have this incredible sense of smell that can be used, both when we hunt to find food and also to guard against predators’. And the humans were like, ‘that’s a pretty neat skill. Let’s make a deal - we’ll give you some of our food, if you can use your skills to help us sleep peacefully at night and hunt better.’

And so began a multi-millennia dance that has obviously morphed and changed over time. But in some sense, those two roles, one - being a guardian or providing this service of protection, and two - detection of enemies or predators or trouble, has never really changed. They often intermingle because their ability to detect threats is what makes them valuable as protectors. And downstream in the gene pool you had all these breeds that developed as a result of adapting for these different roles in human society.
It’s crazy that for all the sophistication and technological development of our time, we still use dogs on the battlefield, in armies, in farms, at airports and borders around the world. Canine units cannot be replaced, because the top dogs are still the top dogs when it comes to detection.
One last question on this - the ability to sniff out organic compounds is clear, but how does this ability manifest in the case of bomb detection?
In some senses, the scent of explosives is easier to detect. Because they are composed of only a few different compounds. Take something like Semtex, which is a type of explosive, which is basically made up of five compounds that dogs can pick up pretty effectively, pretty quickly.
It’s worth mentioning though, on the battlefield, you’re dealing with a whole bunch of other variables. You’re dealing with chaos. Other than just detecting scents, you’re also in this super stressful terrain. There’s explosives, there may be gunfire, there’s all kinds of things happening. The stakes are super high. You can’t really afford to slip up. The handler and the dog are the ones saying ‘it’s okay to come this route, because the dog is sniffed, and there’s nothing there’. You’re trusting your entire unit on the dog.
That’s what Itamar basically had to do. He trusted his life and the life of his unit on the dog’s nose in these stressful conditions on the field. When it comes to detecting diseases, our dogs are in the AC, working for 30 minutes a day in exchange for treats. It’s like a white collar dog’s job.

But our dogs also have to deal with a more complex scent, to be fair. So it’s much harder in terms of acquiring and consistently detecting that signature.
IV. Dognosis
Right, getting back on track. Take us back to the summer of 2023 after you and Itamar had gotten your second EV grant. What were the steps to making this a company?
Itamar and me met for the first time in person Chennai in August of that year, at the 2023 edition of the Emergent Ventures Unconference. He had the same reaction I had the first time around, of just being inspired around all these young, crazy people doing audaciously ambitious things. It was great to meet him there and crystallise our partnership in an environment that helped to make us naively ambitious too.

Naive because, we had received a $25,000 grant from EV. We thought that was going to be more than enough to build a team, set up like a lab, run this clinical trial, complete it, and finally enter the market. That was definitely naive. But it was good to start off with boldness and excitement instead of fear or pragmatism.
We arrived in Bangalore in November of that year and began looking around for a place to set up shop. Naman from Airbound had put us in touch with his broker, who found us a site right next to theirs in Bommasandra. We signed the lease at the end of 2023 and started retrofitting this warehouse garage, basically, to be an office slash medical lab slash dog kennel complex, right next to a neighbour that was trying to build the world’s most efficient drones.

For people who don’t know where Bommasandra is, it’s in the industrial south of Bangalore close to Hosur and the Tamil Nadu border, and it’s really the worst place you could think of setting up if you were trying to do what we were trying to do. It’s mostly a bunch of factories and bad roads and trucks, but the rent was cheap and there was something romantic about starting this off in a garage. That kind of origin helps you build character and you tend to look back on those days with a lot of nostalgia.
Was it just you and Itamar there? How did you staff the initial team, from both a people and, uh, a dog perspective?
Aside from Itamar, we had another dog trainer that Itamar had met while visiting a dog shelter. Then we had a data scientist with a background in cognitive processing and neuroscience. And then we had a bunch of talented interns who were all engineers - mechanical, electrical, software and machine vision. These guys all eventually came on board full time and are some of our most important people today. But that was the initial team. It was a couple of full time people and a crew of interns to get things going.

With the dogs, we adopted two dogs from a shelter in Bangalore. One was a labrador, and the other was a mixed breed between an indie street dog and a lab, named Chloe. We would have liked to staff the entire canine team from shelters because that’s a win-win for both dogs and humans - because we can provide a safe and stress-free environment more suited to their wellbeing - but those dogs have often been through a lot of trauma or injury, so they’re often difficult to train. The two we adopted hadn’t been through any intense physical trauma, though they had been abandoned by their previous owners. For the rest of the team, we found this hobbyist breeder who loved beagles and was going about things in an ethical way, and he was excited enough by the project to let us adopt six of his beagles.
That was the full team - eight dogs and six humans who started off his journey in 2024. We also had a full time caretaker who lived on site to take care of the dogs. So the set up was this large grassy yard where we’d built a bunch of kennels for the dogs to hang out, along with a rudimentary version of our training infrastructure. This was basically a simple platform with eight ports (i.e. holes) in it where you could place a plastic cup.
The broad idea was that in each of these cups, we would place face masks, some of which were from people with cancer, and some which weren’t (to train the dogs to identify the scent of the disease). The dogs would be rewarded with a treat from a central dispenser if they identified these correctly. Itamar’s previous experience also gave him the ability to read the behaviours and body language of the dogs to sense when they had detected something meaningful. We had to lean on that because we hadn’t built out any of the other equipment, headsets, smart suits etc at the time. That was basically version zero of our set up.
Weird question before diving into the actual methodology - would ‘any’ dogs have been a good fit for the task? I remember meeting a lot of beagles when I visited last year.
Well, there was kind of a selection process. We couldn’t just pick up any dog, because what you’re looking for is a dog that actually likes to sniff and play around. We also wanted dogs that would be naturally motivated just by food to then sniff some more, so a passion for sniffing and a passion for food were the two main requirements, which as you can guess applies to a lot of dogs. Not all dogs, but definitely a lot of dogs.

Today we work with both shelters and ethical breeders around Bangalore. Right now we have 15 dogs on the team and about 11 of them are beagles, four of them are other breeds. Beagles just tend to be really passionate about sniffing and eating. They fall on the extremes of both. They’re also kind of independent minded and they have a personality that tends to be really good for this type of work. They’re not particularly fussed about humans, like when you hang out with our beagles they’ll come to you for a few minutes and then they’ll just be amongst themselves. So they work out pretty well. But other dogs are great too. For example, Chloe performs at par or even better than our beagles. So we do think most dogs can be trained to do this.
Outside of the main selection criteria, then you also try and select for a few traits which are more subtle, that Itamar was good at picking up just by watching a dog interact with its environment, seeing its drive, its playfulness, how timid or not timid they were, how they followed their nose - these few different traits that can tell you a lot about the dog’s character.
So originally we did actually see a lot of dogs and picked only a few. This group was already primed for the task at hand, which is essentially to play a detection game that rewards a dog with a treat for finding the target, i.e. sniffing and identifying the right scent. It’s not an easy task, especially with the kind of ‘target’ we were working with, but that’s the fundamental principle.
I’m going to do a terrible job of articulating this, but how did you know what to do? How did you know what to build, what this ‘infrastructure’ needed to look like to see this vision come to life?
I think knowing what to do was something that both me and Itamar have been always pretty clear on. It’s now been more than three years since we started talking, and we’ve not really strayed away from the original idea. There’s been a lot of iterations, there’s been a lot of learnings about the complexity of certain parts of this, or the sequencing of events, there’s been a lot of unknowns to solve with regards to actually implementing things. But the core idea has stayed the same, which is: you want to design a set of sensors, tailor made for a dog, in a way that non-invasively captures as much data on the dog’s cognitive processing as possible.
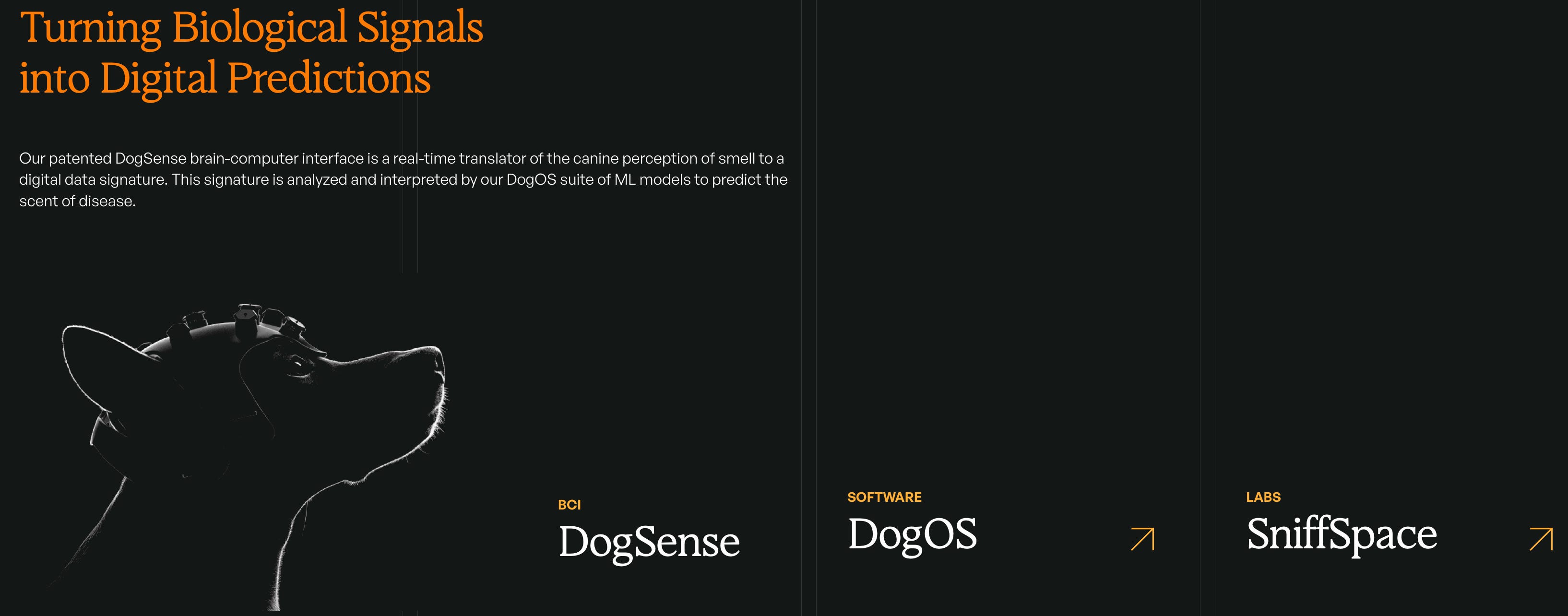
What that translates to is building a helmet that measures EEG (electrical activity in a dog’s brain); building a smart sensor suit that measures respiration, heart rate, and movement data; you want a camera set up that can record their body language; you need software that can digest and make sense of this data; you want a platform where you can conduct this sniffing game, and you want that platform to be as automated as possible, so this process can be smooth and efficient and as free from human bias as possible. We've also built in IR sensors at each port that log exact timestamps of every sniff event as it happens, so you have precise data on when a dog's nose was at which sample, not just an overall session record.

Because of his past experience, Itamar had a lot of thoughts and ideas already about how to optimise this set up for a dog’s experience. What we’re essentially building is an Xbox-for-dogs.

It’s basically a game - an odour detection game that taps into the normal behaviours of a dog. And then you also want to be rigorous with that set up to ensure it can be medical grade, at par with the standards of any other clinical trial, because you’re conducting tests that will impact people who may (or may not) have cancer. So that means samples need to be contained and isolated from each other, everything needs to be well structured and standardised etc.
Got it. What were you actually ‘testing’ - what was in the samples?
Well, we already had the knowledge that you could train dogs to detect diseases from odours, and in fact multiple cancers just from odours. Breath was the most potent and logistically easy discharge to collect.
Essentially you take a regular face mask (the thing we all wore in COVID). People wear it for ten minutes, and that’s it - it now contains traces of their VOCs that are detectable to dogs via scent. You keep that face mask in a Ziploc bag, and then ship that Ziploc bag to a centre where we pick it up to be used in our tests. The dogs can actually sniff that face mask and tell if there’s cancer signals in it.
Our first step was to collect samples from people who had been diagnosed with cancer, who hadn’t started treatment yet. And then we also collect face mask samples from people who don’t have cancer - that’s the ‘control’ set. What we hoped to do was train the dogs to tell the two apart, to be able to identify the masks with traces of cancer.
This basically constituted our first clinical trial, which we ran with local hospital partners in Hubballi including Radon Cancer Centre, Karnatak Cancer Therapy And Research Institute (KCTRI) and the Karnataka Institute of Medical Sciences. The objective was to show that dogs can detect cancer when we know it’s present. In this process, you’re also capturing data on the dog, you’re training models on that data, you’re tweaking the design of the platform, you’re finding ways to automate everything. On the whole we mostly knew the direction we needed to go in, and we got good at handling the implementation problems as they came up along the way.
For the overall set up - was the approach to build all these different components of the ‘solution’ at once? Or did you tackle these one at a time?
The approach we took to this was a little counter to a lot of the startup advice you hear - which is like ‘focus on one thing and do that really well’. We knew that doing the ‘one thing’ wasn’t enough - this whole thing needed to work as a system. You needed sensors for the dog, you needed models reading from the dog, you needed this platform so you could run experiments, you needed clinical samples coming in at the same time because otherwise what are the dogs being trained on. We needed to orchestrate all these pieces to happen essentially at the same time. It many cases that meant starting with a dumb prototype and graduating these to something better whenever it was possible.
I’ll give you a couple of concrete examples. For the EEG, I knew from my time at Berkeley that you couldn’t just tape an electrode onto a dog’s head to capture its brain activity. What you really need to do is design a comfortable helmet for the dog that doesn’t interfere with them or distract them while they’re roaming around sniffing things.

You need it to be snug enough that it collects useful data. But how do you even do that? Dogs have pretty weirdly shaped heads compared to humans. The ergonomics are challenging, like, there’s no natural place to fasten a strap. But all of this needs to be safe and non-invasive, so that was a major engineering challenge that we cracked after a lot of testing. It involved creating head models of the dogs using photogrammetry.
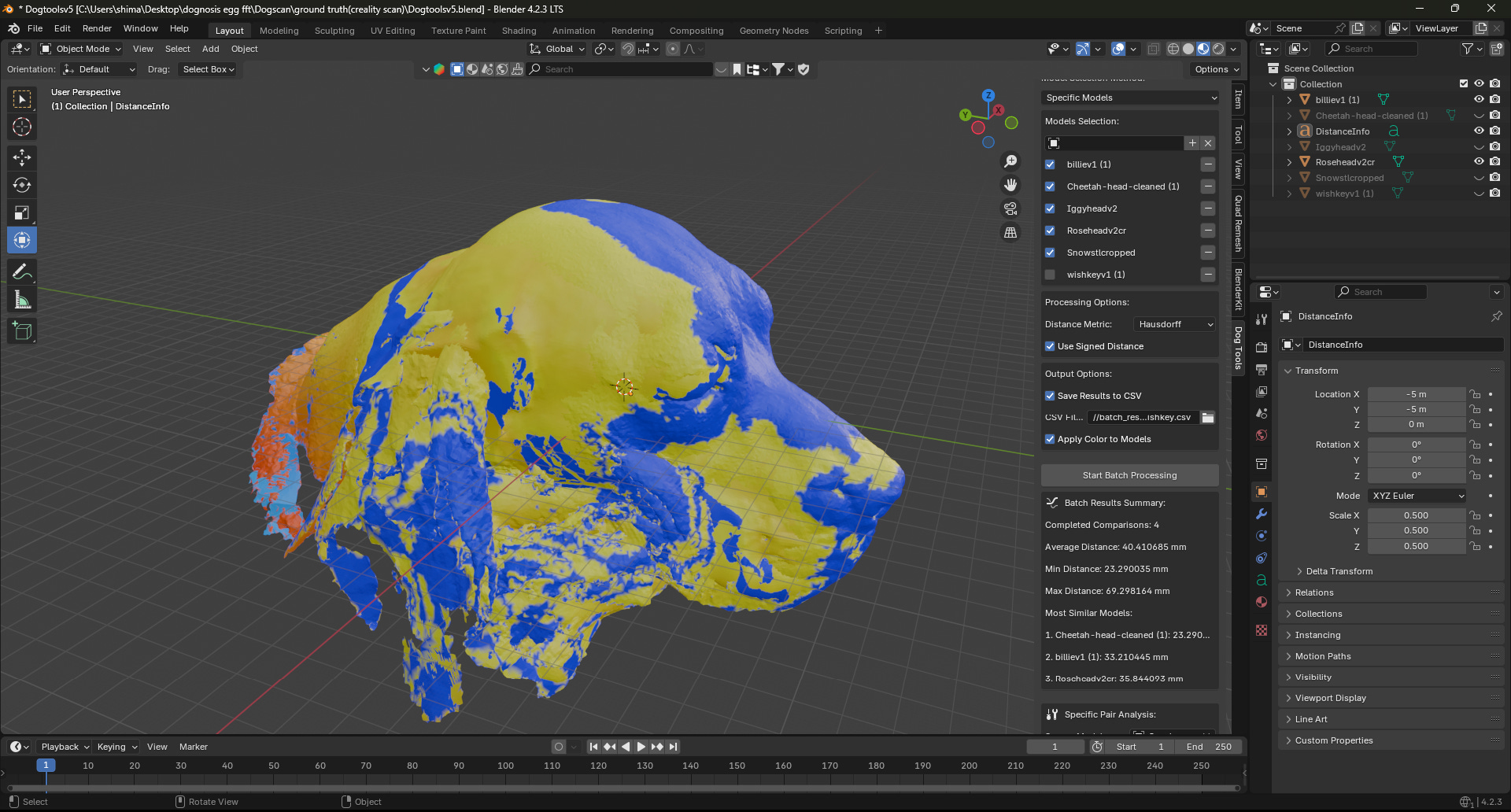
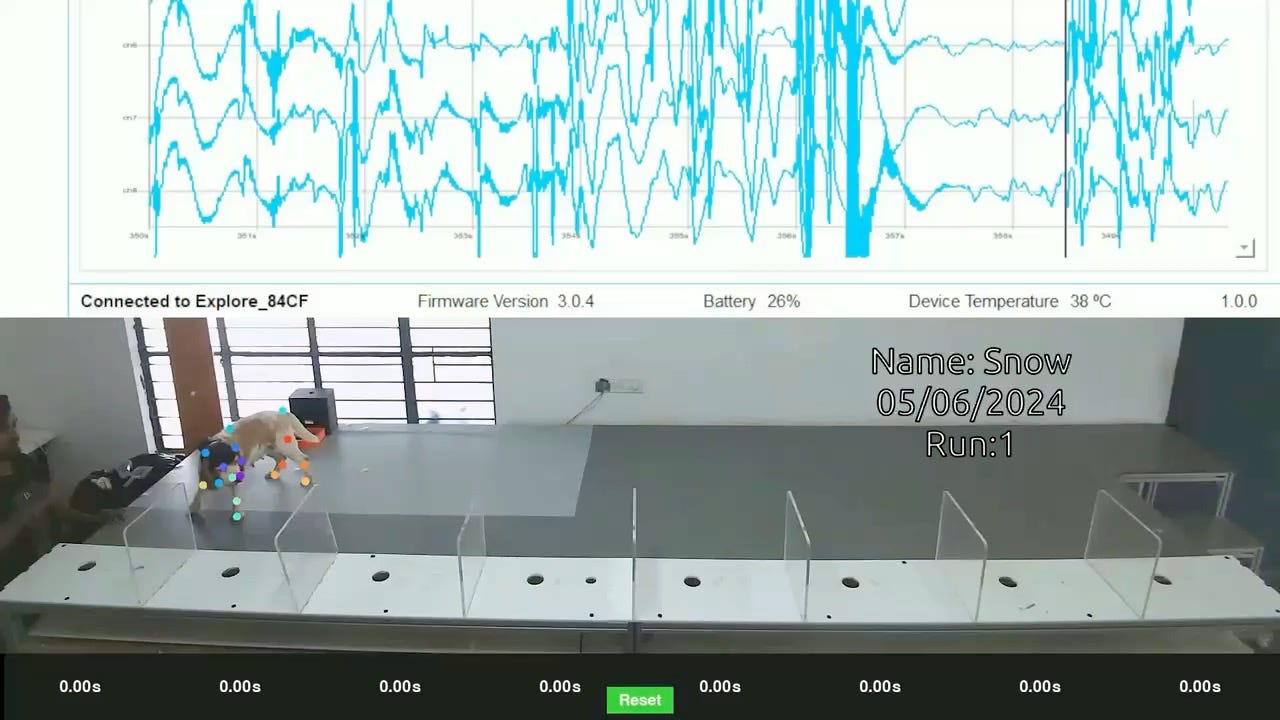
We had people creating sculptures of dog heads and sculpting helmets onto these. We would then 3D print these out and figure out how to make them comfortable. One of the dogs on our team - Snow - she’s like our lead tester. She’s super chilled with anything as long as she gets treats and pets. She had to wear a bunch of weird helmets till we got it right.

Maybe even harder than that to build was the software. As you can imagine, there’s no biomedical disease detection dog software that you can just buy off the shelf. So we had to literally build the databases that allowed us to connect clinical samples to training sessions and then sensor data from the dogs and then correlate all of this in architecture that enabled us to train models to perform both in real-time and post-hoc. It was a tough recruitment challenge to find strong developers who could envision this, but now we have a great team. There’s still a lot to fill in on our roadmap but we’re in a good place now.
So just like this stuff, pretty much everything we do is built in-house except for the EEG amplifier i.e. the electronics for the device that measures the brain waves. That’s only because we have human EEG systems already so we felt no need to recreate that. But the headsets, the platform, the dog training, the testing operation and the whole clinical research side of things, everything is done in-house. There’s no other way to do it if you want to create a synchronised system.
I suppose the larger point is that the main challenge with building Dognosis is that each of these core components is made up of a completely different set of problems requiring a completely different set of skills. We simultaneously need dog trainers, clinical research coordinators, hardware engineers, ML specialists and software engineers to bring this all together. But that’s the only way to do it if you want to actually drive this space forward.
This sounds like a lot to execute just on the back of grant funding. Did you have some more help along the way?
Yeah, after we signed our lease in December 2023, we were lucky enough to get introduced to these two deep tech VCs in the US - Boost VC and 1517 Fund - who specialise in funding crazy ideas, especially at the pre-seed stage. They love backing sci-fi ideas, and our idea sounds pretty sci-fi when you first hear about it.
It’s funny, because I actually think what we do is the opposite of sci-fi. To us this feels like a very natural and obvious exercise - we’re working with ancient technology, something that we’ve known has worked for millennia. All we really have to reckon with is an engineering problem of how to scale, standardise and eventually reverse engineer the nose of a dog. We’re leading with intuition but building on fact, and it was great to find partners like Boost and 1517 who saw the sense in our vision. It was their initial tranche of money that allowed us to hire the right people, and build all the infra we needed.
V. Testing
For someone that has never been to the facility, can you explain what’s actually happening in your set up?
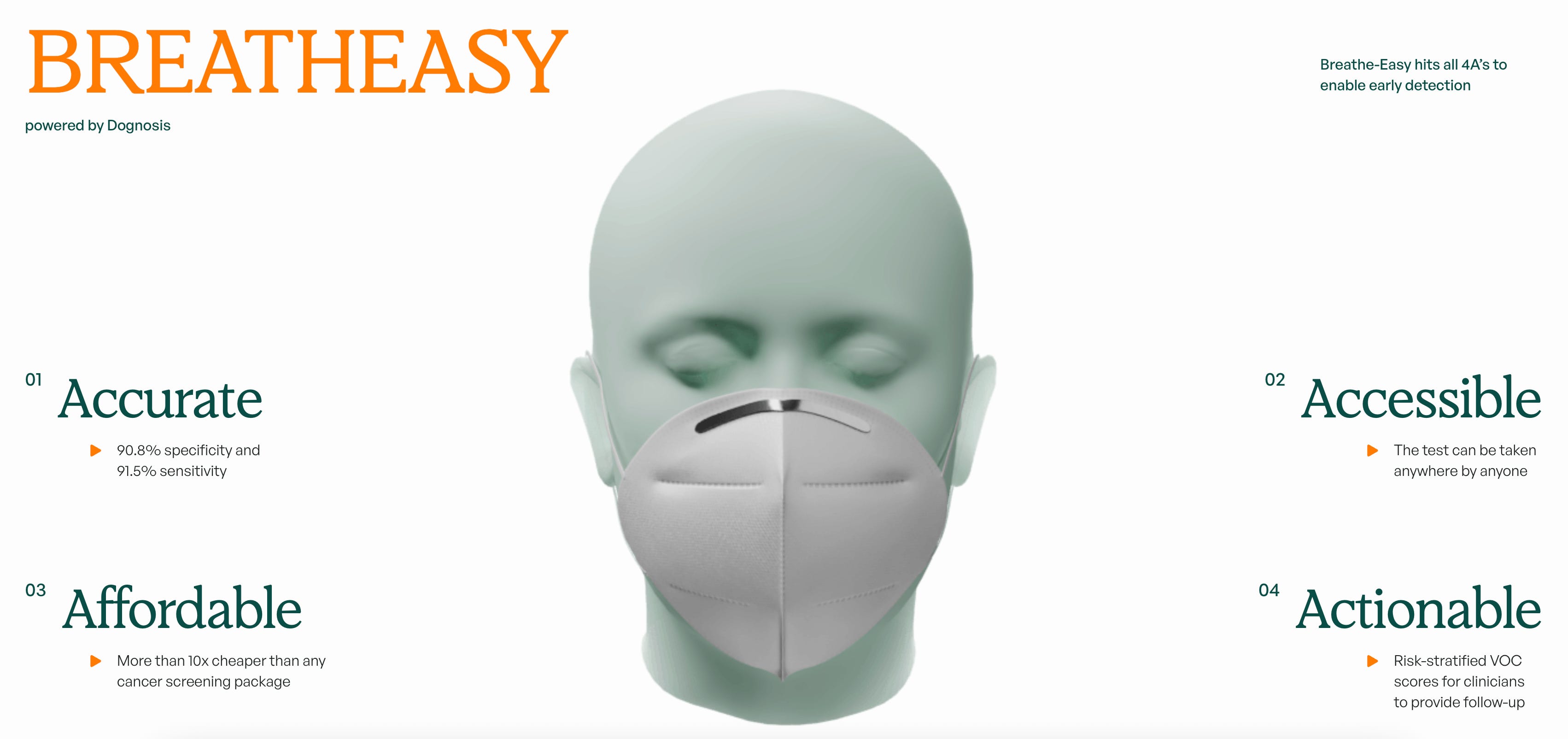
It’s pretty simple actually. Right now the process revolves around our first product offering called BreathEasy. It’s a non-invasive, breath-based health monitoring tool that generates a VOC risk score. It isn’t commercially available yet of course but it’s been the focus of our early pilots with healthcare partners.
It starts with anyone in India breathing into a regular surgical face mask. They’ll wear it for ten minutes of normal breathing - what we call tidal breathing, just your regular breath, no special effort required. The mask is then sealed in an aluminium barrier bag with a QR code, under a documented chain of custody, and shipped to our centre in Bangalore (right now that’s just one centre, hopefully it’s many more in the future). The sample stays biologically stable for up to three months after collection, so it can theoretically travel to us from anywhere in the world with a long window for us to work with. After it arrives, we aim to turn around a report within one to two weeks.

Once that sample comes to us, we place that face mask in a sealed container underneath one of the eight ports on our specially designed platform - which we call SniffSpace. Then a team of dogs - at least three - will come onto the platform one at a time wearing a smart suit each: a custom-fitted EEG helmet and a harness with sensors measuring heart rate, respiration, and movement.

Each dog sniffs sequentially through the ports. When it finds what it considers a positive, it goes back to a central reward station and gets a treat from an automated dispenser. That’s the whole experience from the dog’s perspective - finding the target scent and getting rewarded.
From our side, while this is happening, the system is running at full tilt. Multiple cameras are tracking body language and sniffing dynamics. The EEG helmet is recording brain activity at eight channels and a thousand hertz. Respiration and heart rate are streaming in continuously. And infrared sensors are logging exactly when each sniff event occurs. All of it is synchronised and fed into a software pipeline. Each dog generates a risk score based on the predictive analysis of an AI model acting on all of that data.
One thing that’s worth flagging, because it matters a lot scientifically - during ‘testing runs’, the handler is completely blind to which samples are cancer and which are controls. QR codes only, no identifying information. We know from the history of detection dog research that if a handler knows where the positive samples are - even unconsciously - that information ‘leaks’ to the dog. The whole system is designed to eliminate that.
Anyway, all the individual dog indications are then integrated to produce a single overall probability score. It means we can provide what is ostensibly a pretty accurate pre-screening tool: if your score is low, you probably don’t have cancer and you can breathe easier. If your score is high, you go for the next level of confirmatory diagnostic tests to either rule it out or confirm it.
The idea is to do this in a way that scales, so people across the world can send us these masks, and with very few dogs we’re able to screen a lot of people, and find cancer at its earliest stage, when it’s still a treatable disease. Because we actually can cure cancer if it’s detected early. We just don’t know how to do this at scale. That’s what we’re trying to change.
When I saw this training set up and the dogs doing their thing for the first time, it was kind of an ASMR-type experience. It felt rhythmic and routine and I was impressed at how precise the set up was. What was the thinking behind this particular configuration of the Sniffspace? Is that how it’s done in other places too?
Itamar had a very strong intuition for how to build it. And a lot of it came from what he’d observed at his previous startup - what worked and what didn’t. Mainly, you need to create an environment that lets the dogs be their natural selves - let them be a little chaotic, but then harness that chaotic energy to build structured datasets robust enough to serve as the basis for providing a legitimate health service.
For example, there’s a version of this that other people do where the dog is mostly stationary and you bring the samples to the dog, so very little movement. We were very sure that wasn’t the right way. You want the dog to naturally search, on a platform that harnesses their natural drive. The UI/UX here at Dognosis is designed for a dog. You really need to think: if you’re designing for a dog, what makes the most sense to draw out their natural instincts?
![r/comics - Some recent dog cartoons rejected by the New Yorker, followed by one that actually made it into the magazine! [OC]](https://substackcdn.com/image/fetch/$s_!JogO!,f_auto,q_auto:good,fl_progressive:steep/https%3A%2F%2Fsubstack-post-media.s3.amazonaws.com%2Fpublic%2Fimages%2F1cdb4ffc-7625-4d49-85db-b1587677cea6_640x640.jpeg "r/comics - Some recent dog cartoons rejected by the New Yorker, followed by one that actually made it into the magazine! [OC]")
Itamar had seen enough to know how to strike that balance. The rest we figured out as we went. We also made a bunch of dumb mistakes along the way, of course. For example, for the physical platform itself, we had originally hired four computer science interns who’d been recommended by someone we met at a hardware meet up. Our thinking was, they’ll figure it out. It turns out computer science graduates have very little idea how to build a mechanical rig, even a simple one. We spent a few weeks with no working platform while we figured out how to get people who actually knew what they were doing.
So it’s been a constant work in progress. But now we can actually say, we have an automated platform that scales what the dogs do.
I would love to go a little deeper on the methodology. So as far as I understand, there’s two parts to this training - first, you’re training the dogs to recognise the scent of cancer, so they know what they’re looking for. And then the second part, you’re effectively ‘instructing’ them to find the face mask samples that have traces of cancer - you’re training them to understand that that’s what you want them to find. Is that broadly accurate?
In some sense, yes. The simple way to explain how we train our dogs is positive reinforcement. You teach the dog that the cancer face mask is the scent with ‘meaning’, the one that gets them a treat.
You do this enough times, teach them how to play the SniffSpace game of finding which mask has that scent, and they get better at doing this over time.
But then there’s a whole layer of nuance and protocols and implicit knowledge that we had to build along the way. Because of one fundamental fact - we don’t know what the dogs are smelling. That’s the whole premise of what we’re doing. We don’t have machines sensitive enough to tell us. So the dog is this oracle. But then how do you train an oracle to tell you what you want to know?
The way we do it is we collect samples from people we know to have cancer, and those are the training samples. In the testing phase we also have known samples as calibration checks, to make sure the dogs are still honing in on the same scent. But because we don’t know the underlying dataset that’s going in, what exactly is in that smell, there’s a lot of nuance and careful protocol-building that was needed to really make this work.
The framing we use internally is RLCF: Reinforcement Learning by Canine Feedback. It's a riff on RLHF - the technique used to train large language models by having humans rate outputs. We're doing the same thing, except the feedback isn't coming from humans rating text. It's coming from dogs rating smells. Every time a dog sniffs a sample and makes a judgment, our sensors are reading that judgment - the brainwaves, the body language, the behaviour - and turning it into data we can train AI models on.
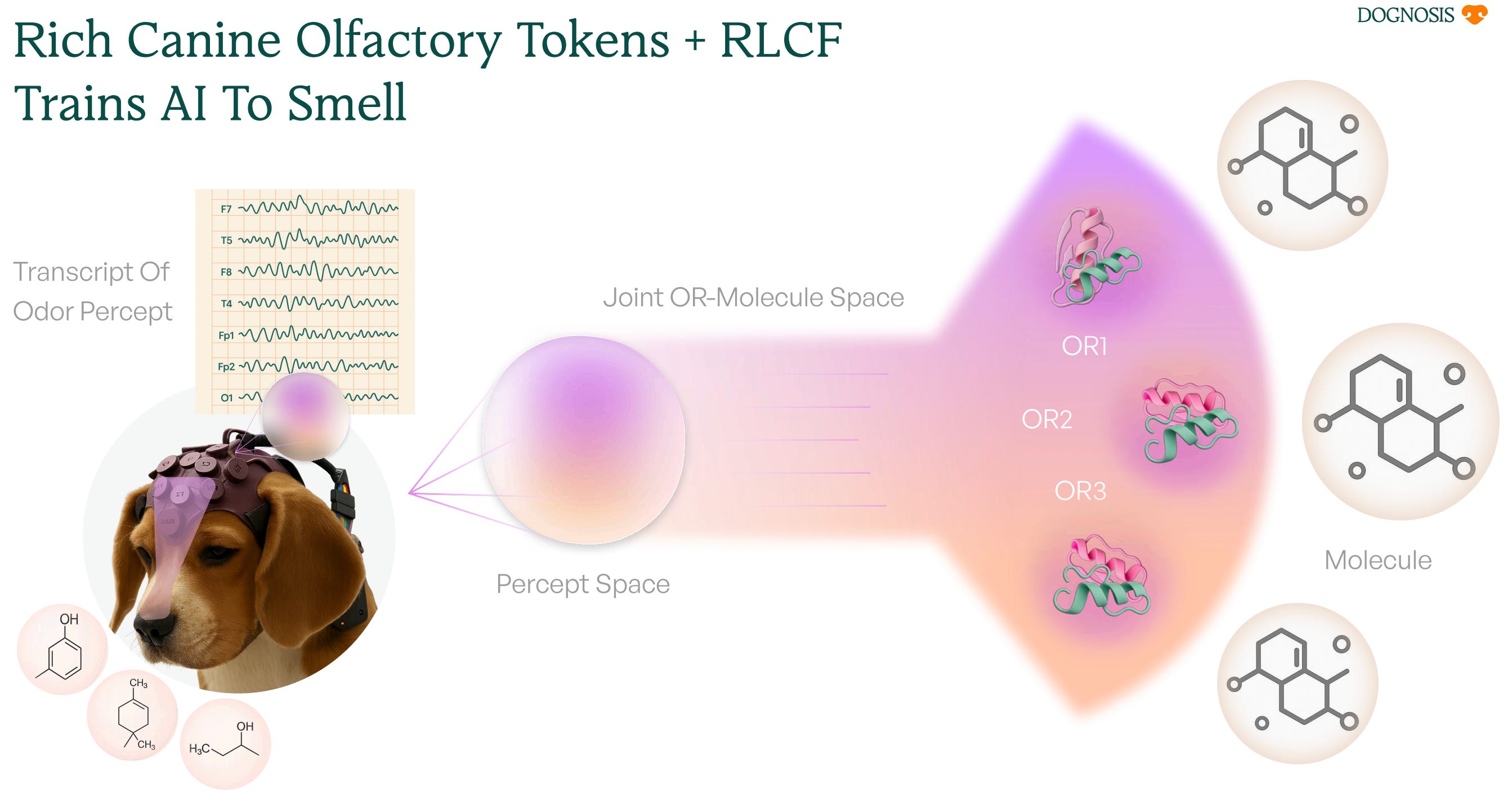
The dog is the teacher. We're building the language, infrastructure and protocols for the AI to take notes
You mentioned that you’re not just recording the electrical signals in the dog’s brain, but you’re also taking into account a lot of other data points on how the dog acts, what’s happening in their bodies, their outward body language etc in order to build a holistic understanding. Can you elaborate on that?
Our goal is less about understanding and more about prediction - that’s where we’re currently at. We might still not know how the dogs are doing what they do, but now we can predict whether they’re smelling a cancer sample versus a control, because we have enough data from past instances of both, and we have the signatures that corresponded to those events. In other words, we don’t need to solve the full scientific mystery of what the dogs are detecting in order to build something that works. We just need to be able to read them reliably, that’s why we take all these different inputs into account. So we’re in the business of prediction right now.
The way we build these multi-modal prediction systems is to say that each stream of data, whether it’s from the dog’s brain, from their heart, from their respiratory system, from their movement, or from their body language as analysed by cameras, each of those streams is giving us a part of the equation. The EEG helmet captures what’s happening neurologically in real time. The respiration sensor picks up changes in breathing pattern that the dog itself can’t consciously control. The cameras read the body language. We have all these streams and integrate them in an overarching system (that we still need to do a lot of R&D on in terms of how best to interpret everything). But each of them is giving us signal, and each of them is making our predictions better.
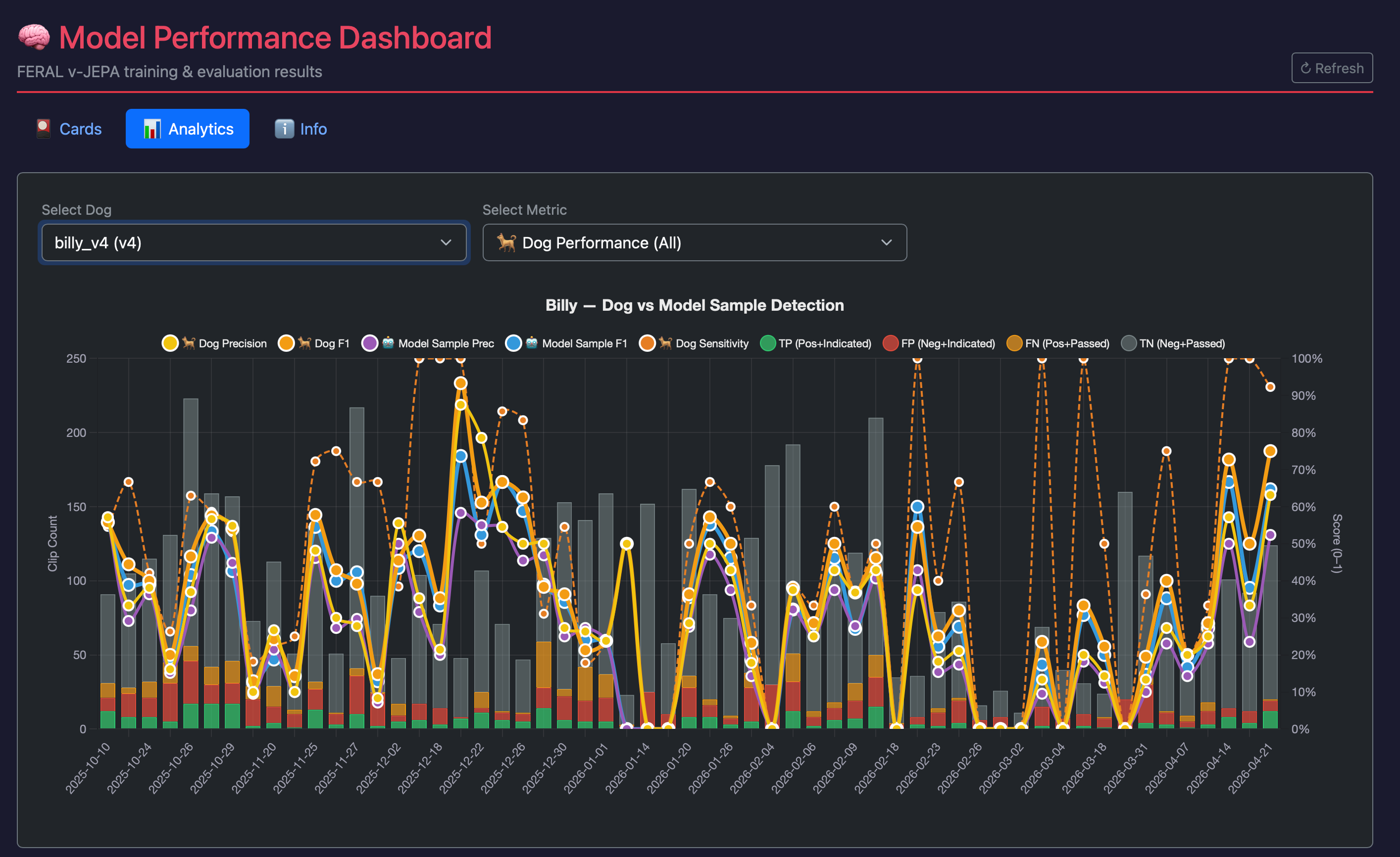
Even with vision models alone, which have become very powerful in the last five years, just using camera data of the dog’s body language, we’re actually able to match what a human trainer can do. From the dog’s body language we can tell if they’ve just sniffed a cancer sample, the same way an average human trainer could from looking at the dog, because ultimately both the human and the camera are doing the same thing - looking at the dog and reading what it’s probably smelling.
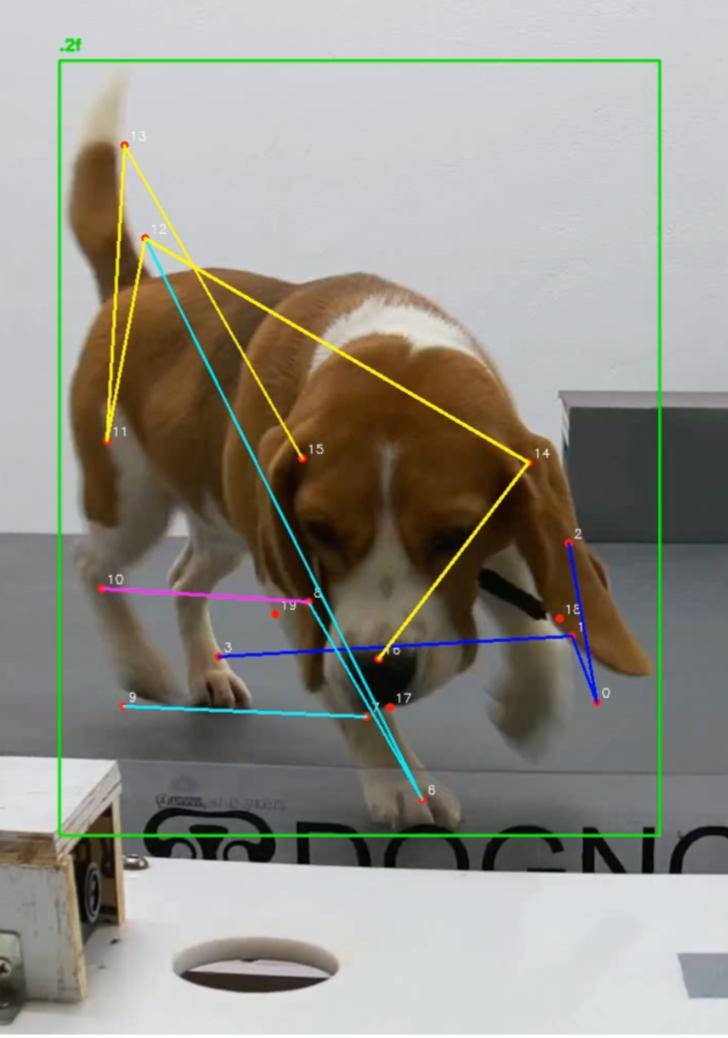
This is important because it means the system isn’t dependent on having an expert handler in the room. The model learns to do what Itamar does, and eventually to do it better. The first goal is to match the capabilities of an expert trainer like Itamar. And then the final step is to create a superhuman trainer, one that can read signals that humans simply can’t, but that are actually present if you could read the dog as well as it’s possible to read them.
So if you had to run this training and dog-translation autonomously - what would that look like? Is the idea that the dog would walk on the platform wearing the smart suit, it then sniffs a bunch of ports with samples with no human present, and then as the dog sniffs and makes a decision whether that sample is a cancer sample or not, the computer records it and you repeat the process?
Yeah so you rotate a disc under each port to switch samples, so the dog walks in a circle sniffing its way through them. It walks for ten, fifteen, twenty, thirty minutes and has evaluated hundreds of samples in that time, each one becoming a data point of what the dog thinks that sample is. All of it gets stored in a structured database that you can aggregate across dogs and then generate a final risk report from.
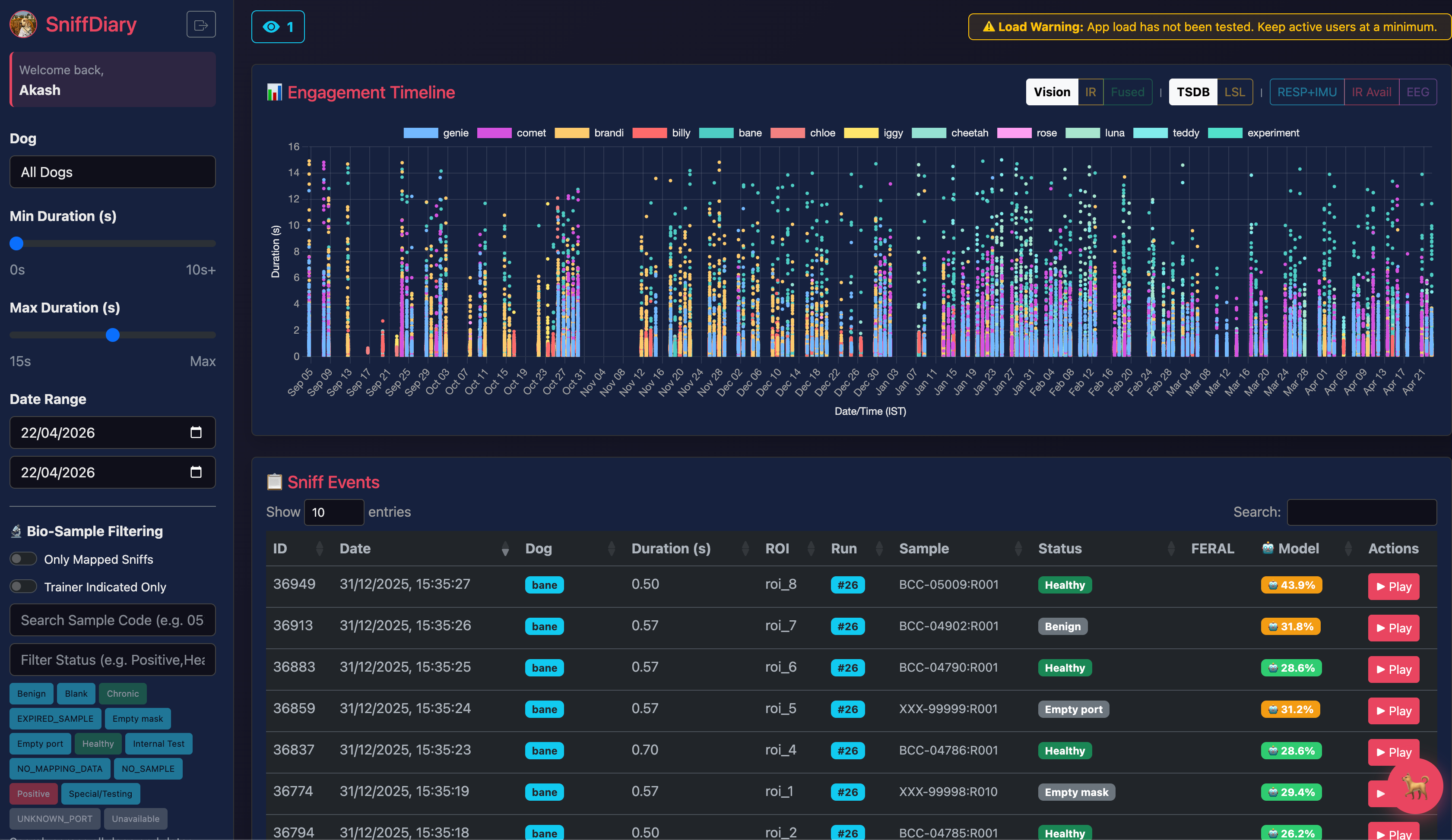
None of this requires a trained human in the loop reading the dog. And that’s actually the key thing, because the human has always been the bottleneck. Not the dog’s nose. The human who has to interpret what the dog’s nose is detecting.
There are very few people in the world who have actually gone through the professional experience of reading dogs at this level. Itamar is one of them.

That’s partly why having him as a co-founder has been so critical, and also why we can’t rely on people like him to scale this. Humans get tired. Humans make mistakes. And when you have a standardised system you simply can’t afford this lossy communication interface between human and dog. You need something that’s standardisable, where there are no communication errors.
What the AI trainers can do is both train the dog from zero to one, and then during the testing phase constantly read what the dog is picking up in a manner we just couldn’t do before. The dog’s perception doesn’t change. What changes is our ability to read it accurately, consistently, and at scale.
To pick up on that last point again - is all of this to get to a point of first removing the humans from the loop, and then eventually to removing the dogs from the loop too? Is there a world where we can train machines to wholeheartedly do this job once we have enough data?
It’s an interesting question, and something we’ve spent a lot of time thinking about. People often ask us some variation of “well, dogs are surely not the optimal way to do this right? You’d want to replace them with machines eventually, right.” And I often pause on that, because I’m not really sure that’s true.
In some sense dogs are these olfactory supercomputers that have been evolved over millennia to be really good at sniffing things. They have the hardware, they have the software, they’re aligned with humans, they’re happy to do this thing for us without consuming tokens or electricity. They’re down to do it for treats. Is there a better architecture for detecting scent? I’m genuinely not sure. It seems like the dogs are great, and we’ve just not built the right interfacing layer.
That said, there is one thing a sensor could do that a dog can’t, which is give you mechanistic insight. If hypothetically there were advantages to replacing dogs with some kind of sensor, the main one would be being able to say with certainty, okay, these are the specific compounds the dogs are smelling. That would be genuinely useful to know. But I still see the future potentially remaining dog-first. Because in some sense, we already have olfactory supercomputers in most of our homes. You have the power of a full body MRI in your dog. You just don’t have access to that insight yet.
It’s worth mentioning that we are doing some work on this. It’s one of our moonshot projects we're most excited about, with one person working on it full time. The idea is that we have the ability to reverse engineer the cocktail of molecules that our dogs learn to hone in on when imprinted with an odor and you can use that information to build the e-noses of the future.
I’m envisioning something like a portable COVID-era temperature scanner, where you point this device at someone’s mouth and it’ll tell you if they have some disease.
Yeah, it could be something like that. People have talked about how you can build just a module on a smartphone that gives it a nose. You breathe into your phone every day and it can tell you if you’ve started developing any type of disease that has a scent. And we think most diseases do have a scent - from cancer to infectious diseases to things like Parkinson’s and Alzheimer’s, all of them change your scent profile in a way that is consistent for that disease.
If you just had a way to understand what those scents were and decode them, you could build a system where any disease is caught at its earliest actionable stage, while a person is just sitting in the comfort of their home breathing into a device. That could be the long game. The dogs can get us there by teaching us what to look for.
VI. Slaying The Emperor
I want to switch gears here for a bit and rewind back. Obviously you don’t have to justify why you are focusing on cancer. It’s one of the big, open, unsolved questions for human healthcare and happiness. But do you have a personal axe to grind when it comes to the disease too?
I do have a personal axe to grind. My mum’s mum passed away because of cancer. And my mum’s sister’s husband died recently because of gallbladder cancer. Those were close family members. And they likely could have had much better outcomes if their cancers had been detected early.
But in terms of my motivation to build this and focus on cancer, it’s not only that. There is something personal. But there’s also something that is just so common and shared across everyone. Everyone has lost someone close to them to cancer. Everyone has a personal axe. The axe is a common axe that we all have to grind.
My grandmother and my uncle are a personal reason to push harder. But it’s not specific to just them. A lot of people all over the world could have been saved. And that’s the thing about cancer - it’s not a disease that picks its moments or its people. It’s indiscriminate. Which means the solution has to be too. This is one of the hardest diagnostic problems that the dogs can help us on, and it’s the one that affects us all. So it just made sense to start here.
You had sent me this article from Siddhartha Mukherjee on the issues with cancer detection that are still quite prevalent, and how many of the leaders in this market are still operating a very low percentage of accuracy when it comes to detecting cancer, at least at the early stage. Can you spell those out reasons for our readers, and help people understand the crux of the issue?
Mr. Mukherjee is great in that piece. I’m also actually finally reading The Emperor of All Maladies, where he chronicles the whole history of cancer. I’m just envious of his ability to write. It’s an amazing book.

Cancer is basically one of humanity’s oldest diseases. There’s this infamous ‘Case 45’, chronicled by an Egyptian physician almost four thousand years ago, detailing a tumour he finds in a woman’s breast. This is in the context of him writing reports on all kinds of diseases and how to treat them. The Egyptian school of medicine actually had pretty decent answers for a lot of things. But for Case 45, the breast cancer tumour, when it comes to a cure, he simply notes down - there is none. No treatment. And in some sense, even now, when cancer is detected at a late stage, Stage Three or Four, and it’s spread across the body, we have novel immunotherapies and all kinds of things we’ve spent a lot of money developing, but often there is still nothing you can do.
The problem with detecting cancer early can basically be summarised as a recursive needle in a haystack problem. A needle in a haystack is finding a tiny signal in a lot of noise. Finding cancer early is like that - at an early stage you have some clump of cells that has gone rogue and is rapidly dividing, but you have no symptoms until those cells have already infiltrated a bunch of places in the body. That’s when you have Stage Three cancer. You get symptoms, you go to the hospital, and you find out it’s already metastasised. This happens in eighty percent of all cases in India.
Now to find that needle in the haystack early enough to change the course, you need to solve another needle in a haystack problem first - who in the population has an undiagnosed case of cancer right now? Despite being such a terrible disease, cancer is actually not that common at any given point in time. Above the age of fifty in India, roughly one in 150 to one in 200 people will have some type of cancer in a given year. So any test you have needs to test 200 people to find that one person. It’s a needle in a haystack inside a haystack.
This is where you run into the fundamental constraint of any diagnostic test - the balance between sensitivity and specificity. Sensitivity is, if the disease is present, what are the chances of finding it - your false negative rate, how many times do you miss it. Specificity is your false positive problem - of all the people who don’t have the disease, how many will you correctly rule out. If you need to test 200 people to find that one person with cancer, you want a test that does both. Very sensitive so it finds that one person, but also specific so you don’t tell 199 other people they have cancer when they don’t. And here’s the kicker - you can’t fully solve both at once. Optimising for one comes at the cost of the other. It’s not a technology limitation, it’s a mathematical one.
Even today we haven’t solved this for basically any cancer. We have a few screening tests that have seemed really effective, like the mammogram, but even that is very hard to scale in a country like India, and in the west most cancers still don’t have a screening tool that works at a population level. Solving this recursive needle in a haystack problem turns out to be a really hard problem. Which is why Dognosis isn’t trying to solve both layers with one test. The dogs solve the first problem - who in the population is worth looking at more closely. Everything else flows from that.
Can you elaborate on this issue in the case of India in particular?
Less than one percent of Indians are screened for cancer in their lifetime. Current methods like full body MRIs or liquid biopsies simply can’t scale. And even the simpler, lower cost tests that do exist struggle, because they still have real problems.
But before we even get into the India-specific issues, it’s worth noting that most cancers don’t have a screening test at all - not just in India, anywhere in the world. Something like ovarian cancer, liver cancer, oesophageal cancer - there’s just no screening, period. You find it accidentally when symptoms develop. You get a stomach ache, you go to the hospital, and you find out there’s a tumour growing. That’s how it goes across the world for a huge proportion of cancers. For the ones that do have screenings, those only cover thirty to forty percent of all the cancers that actually occur in India.
And for those cancers, historically India just hasn’t been equipped - we have a huge population, so the needle in a haystack problem is even worse than elsewhere. Cancer is already a needle in a haystack. Now it’s in a massive haystack. And we don’t have the infrastructure to run something like mammograms everywhere. Not that mammograms are the answer anyway - screen everyone with a mammogram and you end up with enormous numbers of false positives, and that’s only for one cancer. All the problems with current cancer screening are just exacerbated here.
There's also just the basic cost factor, and the friction of needing to go to a hospital at all. For a lot of Indians, taking half a day off work, travelling to a facility, paying for a test for a disease you don't yet have symptoms of - it's just not something that happens.

So the acceptability of current tests, the accuracy at early stages, the false positive problem, the recursive needle in a haystack, the lack of resources per capita - all of it is worse in India. And then there’s something specific to South Asian Indian psychology - the stigma and the desire to rather not know about an illness, to deal with the consequences of being sick once you’re already sick, rather than being proactive. That’s something you see especially in villages, where people would genuinely rather not find out they have cancer than deal with what comes after that diagnosis. And the reason for that is the stigma of cancer as a death sentence. Which creates this terrible self-fulfilling prophecy - we don’t screen, therefore it’s detected late, therefore it is a death sentence, therefore there’s more stigma to not screen.
Breaking that cycle has always been the challenge. But we really think if you can solve for the tools - something easy, non-invasive, low cost, that doesn’t require going to a hospital - you at least have a fighting chance of breaking this wheel. And the need is getting more pronounced, because we have all these trends with nutrition and pollutants and pesticide use that are just going to increase cancer incidence further. India already accounts for roughly a fifth of global cancer deaths. That number is going up, not down.
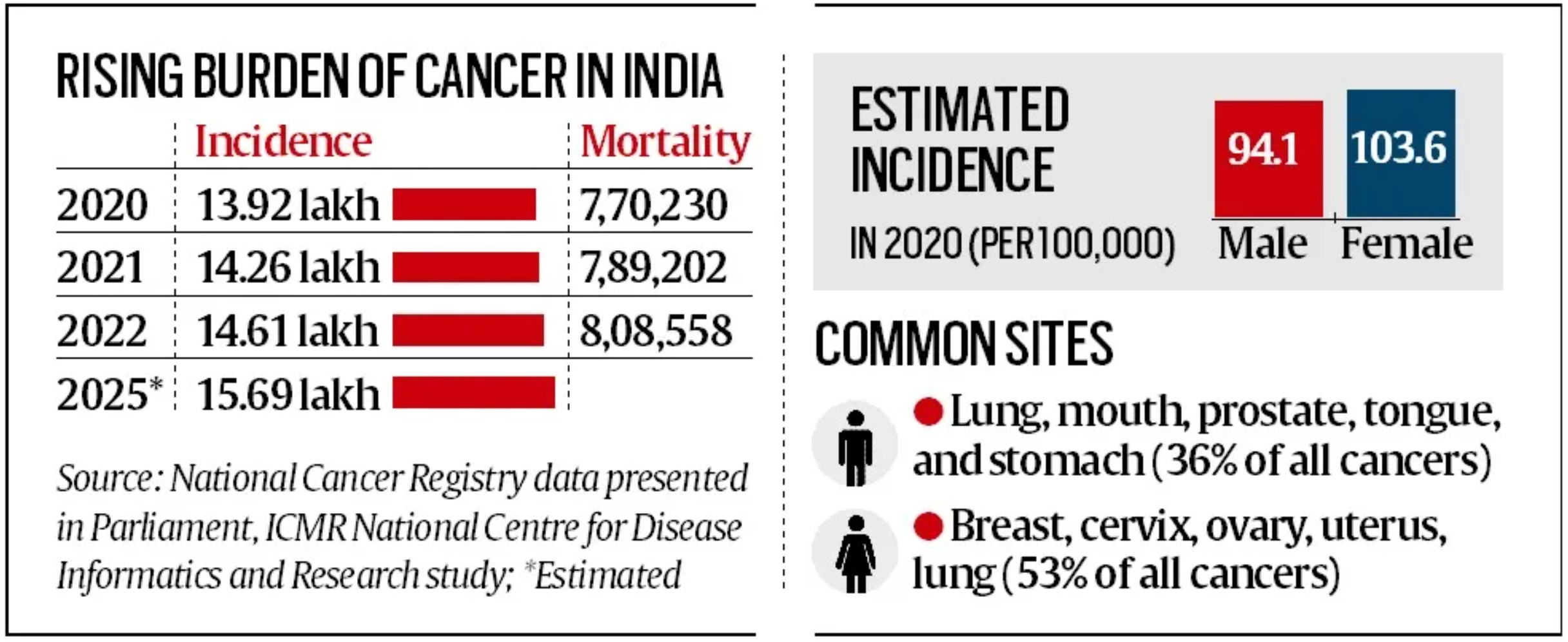
So India is definitely the place where this can have the most immediate impact. But there’s another reason why India is great for Dognosis, and it’s not just about the problem we’re solving. It’s that India gives Dognosis the best chance to actually succeed.
Both the dogs and our machine learning models require two things - data and talent. Lots of clinical samples for the dogs to learn from, and then our models learn from the dogs. And then human talent to build all of this. When it comes to engineers and scientists who are hungry to work on something as interesting and complex and meaningful as Dognosis, India just has an extraordinary depth of that. We’ve built a team of almost fifty people and fifteen dogs. We simply couldn’t have done this at pre-seed and seed stage, pre-revenue, anywhere else in the world. Building all five layers simultaneously - the clinical operations, the dog training, the hardware, the software, the machine learning - none of that would have been possible if we weren’t in India.
So Dognosis is best built in India. And the solution we’re building is best applied to India first. It’s a compelling reason to be here on both counts.
Why is the way you guys are doing it so much superior to the ways the other companies and entities in the world are doing it - that goes for the use of traditional diagnostic techniques as well as the dog-supported pre-screening tools?
We don’t necessarily think we’re superior to the current tests. We think we’re solving the problem that needs to be unlocked for those tests to work.
If you have two needle in a haystack problems, you need two solutions. It’s a funnel. You first need to solve for which person in the population likely has undiagnosed cancer, and then for that person you figure out where the cancer is and what kind it is. So far what everyone has been trying to do is solve both of these problems with just one test. And that’s impossible, because of the statistical problem we talked about - you can only optimise for one of the two, finding cancer or ruling it out.
But if you have a system with this funnel framework, your first test identifies who in the population is likely to have cancer, and your second test focuses on finding the cancer in that much smaller, much higher-risk group.
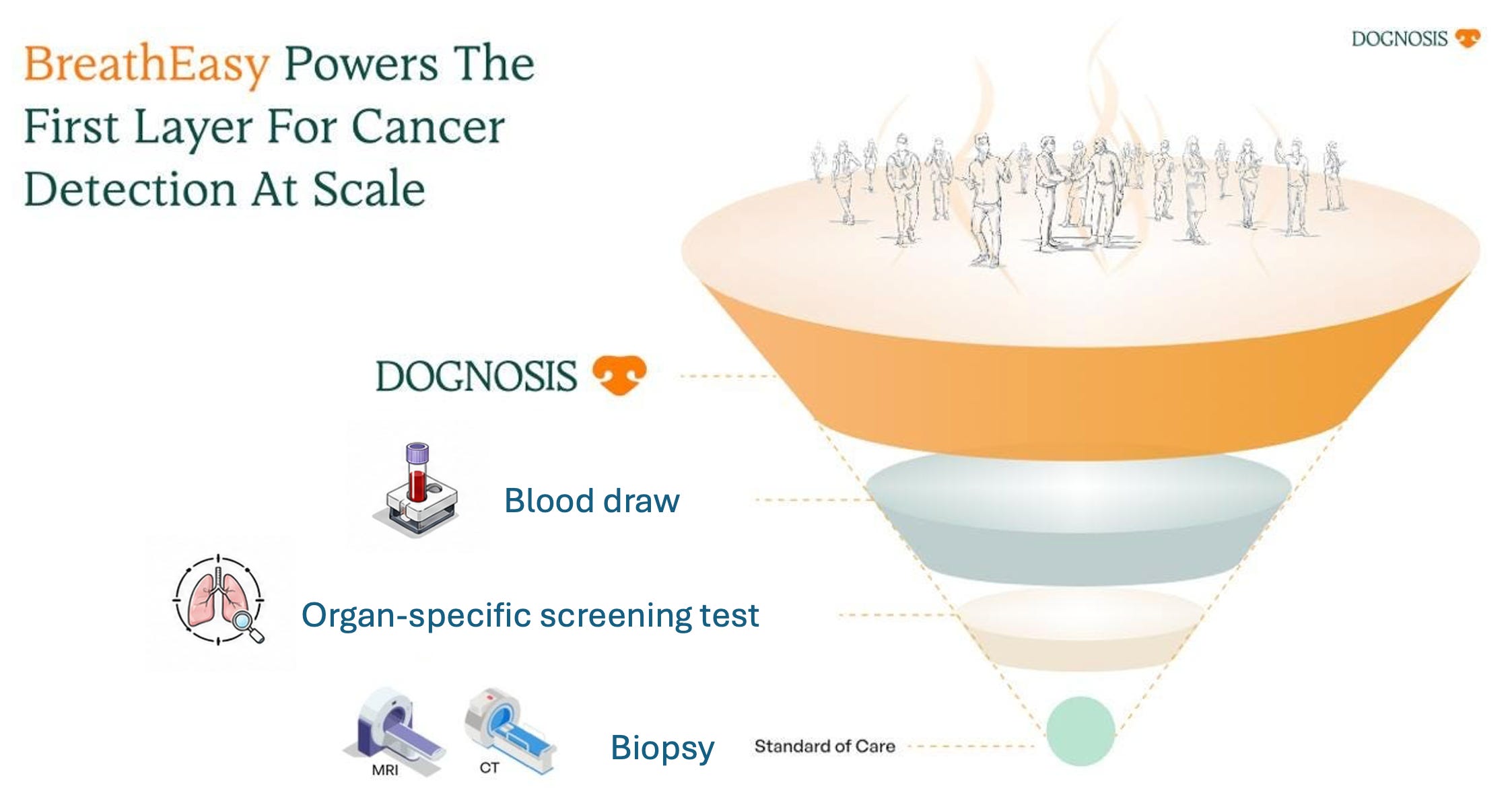
What the dogs have always been great at is solving that first problem. They bring their nose to the haystack and the nose has a magnet, and the magnet attracts the needles. They can sniff hundreds of samples in a few minutes, and because their noses are so sensitive, if cancer signals are present they identify it, in a way that’s simply not cost effective with any other test.
So the dogs take out the hay from the equation. Any of the people they flag as higher risk can then have the tools we already have today - liquid biopsies, organ specific screenings, full body MRIs. But now those tests are focusing on a much smaller group of people, and suddenly they can do great, because they’re focusing on the problem they were actually designed to solve. A liquid biopsy with fifty percent sensitivity across a general population becomes a very different and much more powerful tool when it’s running on a population that’s already been filtered to ten times the cancer prevalence.
What we’re doing is adding the piece that’s always been missing and complementing everything else. It’s a systems approach to a problem that has always been attacked from one angle. And the dogs have just been so underutilised in all of this - regarded lower than underdogs. They’re just not treated with the respect or the gravity their abilities deserve. They can actually solve this problem - we trust them to solve this problem.

What’s been missing is a way to standardise and scale what they do. That’s what our technology uniquely allows - AI trainers and a robotics platform that can run autonomously without a human in the loop, doing this at scale.
VII. First Paw
Ok I want to return to home base. I think our readers will now understand what you’re doing, why you’re doing it, and how you’re doing it. But, does it work? You started this journey off in a garage in Bommasandra in late 2023. Has there been a big breakthrough moment, a moment of validation?
The big milestone was June of 2024. We ran a small blinded trial - a blinded trial is where we didn’t know which samples were the cancer samples and which were the controls. We just had QR codes. We basically blinded ourselves completely, and then we ran the dogs on our first gen platform, where a handler was interpreting the dog’s behaviour directly. We had prototypes of the EEG helmet and the sensors by then, but they weren’t at the level where we could actually use that data yet. It was just the dogs and a human reading them. The dogs had seen about 800 samples by that point in the first few months of 2024.
In the blinded trial we had 200 samples - 25 from people confirmed to have cancer, 175 that were controls. Six dogs ran in the study and we planned to analyse their performance after the trial. It turned out that out of 25 cancer cases, the dogs identified 24 directly. They missed only one. Out of the 175 controls, 96 percent were correctly rejected as not having cancer. So the overall accuracy around 96 percent too. And this held even for the early stage cancers - we had a few, not many, but enough to show that both early and late stage were being detected accurately.
Even though it was a fairly small trial, it was still one of the larger ones conducted at that point with breath and multi-cancer. For context, most published detection dog studies at the time had fewer than a hundred participants. We had two hundred, across multiple cancer types, in a properly blinded setup. That data became a white paper, and was presented the following year at ASCO 2025 - the largest oncology conference in the world.
So at that point, already, we had built a system from scratch that could hit this accuracy. 96 percent is better than most diagnostics. And that was a turning point for me like - wait, this is real. This is no longer an idea or an academic paper. We are actually detecting cancers in the real world, with a system that we believe will scale as we build the missing pieces.
Man, what was that day like?
Chaos. We tried our best to run a gold standard trial and the data was robust, but it was also complete chaos. Remember, this was a garage where I was running a lab, an office, and a kennel unit all in one. It was pretty stressful.
I remember doing the analysis that day. Our software wasn’t fully ready yet - we had all the data but there was a lot of crunching to get it right, and the cloud wasn’t cooperating either. There were moments that day where I genuinely wasn’t sure the numbers were going to come out the way we hoped.
But once we summed it all up - the dogs had achieved 96% sensitivity, meaning if someone had cancer and had given their mask, the dogs caught it 96% of the time. And they had achieved this with just ten weeks of training on around 800 samples. It didn’t take that many days or samples for the dogs to get really good. Which in itself tells you something about what they’re capable of.
The overriding emotion - and this is true of all the milestones we’ve hit since then - was just: cool, now let’s keep going. There’s a moment of celebration and then you look up and the harder parts are already visible.
So this was June 2024, what was the next step?
So June 2024 was the small trial - 200 participants, 25 cancer, 175 controls, 96% accuracy. But that was the interim dataset of a much larger trial we’d been working on with 1,500 individuals, about 283 of them with cancer and the remaining controls. That completed in June 2025 and was published in the Journal of Clinical Oncology. And there we retained about 90% accuracy, both sensitivity and specificity - fewer than ten percent false positives or false negatives - across a bunch of different cancers, all quite adequately powered in terms of sample size. That’s the largest breath-based multi-cancer study ever published, and the first to show this level of accuracy consistently across both early and late stage of the disease.
We also moved the whole setup from the garage in Bommasandra to this two-acre facility that you’ve visited. Setting up buildings, an office in Bangalore, the lab here, strengthening the team. All of that was happening simultaneously.

But more than anything, the focus has been on getting from an artisanal process - human handler, dogs on a platform - to something that is actual infrastructure. Something that can be relied upon, replicated, standardised, regulated, put under quality assurance. Everything necessary to go from the curiosity of dogs sniffing out cancer to the real world implications of what that can unlock. That’s just been engineering and operational muscle development.
We built version two of SniffSpace - automations of sample presentation, keeping samples contained so they can be relied upon for longer periods. Getting the EEG and the respiration sensor, the whole smart suit, from prototype to something more like a product you can use every day with different dogs, retaining good signal, with software that captures all of this, synchronises the timestamps, and feeds into a pipeline that predicts in real time. Really taking the human out of the loop - not just in interpretation but in conducting the sessions themselves.

That’s still a complex challenge. It’s like autonomous driving. Going from co-pilot to fully autonomous. Right now we’ve built a co-pilot for the trainers. Going forward we want to replace them completely - Level Five autonomy for biomedical detection dog training. We’re progressing up the ramps. The machine learning models and the whole infrastructure still need work. But the translation from curiosity to infrastructure is what has really taken up our time, and will keep taking up our time going forward.
And now we’ve also started the prospective trials - testing people with no history of cancer, following up with the positives and a subset of the negatives, and showing that we’ve actually detected previously undiagnosed early stage cancer. Doing this in a way that allows us to make strong claims about how this should be implemented going forward.
Can you tell us more about this study that was just published? What did it show for the first time? What kind of validation did it give you guys?
So like I said that mini trial in June 2024 was always the interim dataset of something much larger. For this one, in total we ended up getting 3,200 plus individuals to volunteer for this study across six hospitals in Karnataka, adding to our roster of partners via strong relationships with the likes of St John's Research Institute, Narayana Health and Aster CMI.

We divided the dataset into a training and test split - the way you’d evaluate any machine learning model. Train on one set, but evaluate on a completely separate set the model has never seen. The test split alone was 1,500 participants - 283 of them with biopsy-confirmed cancer, the remaining controls. We were blinded throughout, same as the initial trial. And on that test split we evaluated the dogs fused with some clever algorithms we’d developed to standardise their performance.
We really wanted to set aside the dismissal of ‘oh these are just small sample sizes, how do we really know it’s true?’. So we went big - at least two to three times bigger than any study that any other labs and groups around the world had done before. We had a very large trial set. We had multiple cancers included, and we did this in India where the real world impact we felt like was most evident. We wanted to prove that you can scale a new system in a country that doesn't really have robust cancer screening infrastructure, and do it in the settings where it actually matters.
A lot of our samples came from community camps - volunteers who just showed up, no cancer history - as well as public and private hospitals across Karnataka. Not a pristine academic setting. Real hospitals, rural catchment populations, the full messy reality of Indian healthcare. It’s really representative of how such a system would actually be deployed.
This dataset, that study, was just published in the Journal of Clinical Oncology - the world’s top cancer journal, the one that basically shapes clinical practice. Oncologists actively read it to update how they think about new lines of treatment and new diagnostics. It went through peer review and was published with a commissioned editorial because they wanted to highlight this study. They’re doing a podcast with us too. They’re pulling all the stops.
The significance of the JCO publication is hard to overstate. This isn’t a niche journal or a preprint. When something appears in JCO with a commissioned editorial, it changes how oncologists think and practice. It moves something from the fringes into the mainstream conversation.
What we showed is that everything we’ve known about the dogs is true, at the most rigorous level of study you can run. 90% plus accurate across over twenty types of cancers, with performance staying consistent at Stage One and Two when it matters most. That sensitivity at early stage is four times better than the next multi-cancer test on the market - from GRAIL and Exact Sciences, public companies worth billions that have invested hundreds of millions in R&D. The dogs just outshine them.
The clinical establishment is finally waking up to the fact that this is a real thing with real possible impact. The dogs will no longer be seen as a curiosity. They’ll be seen as a genuine solution to a real problem.
So what is yet to be proven at this point? Obviously, like you said, there’s now validation beyond fascination and curiosity and gimmick, there’s real scientific grounding underneath the disease detection abilities of these dogs. But what do you need to still demonstrate?
All that being said, we’re also very aware that this is not the final end-all be-all, and that we can’t just go to market and start testing people.
What any rigorous evaluation of a cancer screening test needs to prove is that it works in a prospective manner. Prospective means you don’t know the labels of the samples you’re collecting. You don’t know what’s a positive and what’s a negative. You just have a sample from someone who’s healthy, no symptoms, no prior cancer history. And based on your test results - positive or negative - does that actually predict their true status, as confirmed by gold standard detection?
That kind of prospective validation is necessary before you can truly say your test can be applied on a population level. Any rigorous researcher or clinician would want to see it. And it’s what we know we need to do.
So that’s the next step. We know dogs can detect cancer when we know it’s present. Now we need to show that it works when we don’t know it’s present. That’s a fundamentally harder problem, not because the dogs are any less capable, but because the math changes completely. In our Phase-2 study, about one in five participants had cancer. In a real screening population above the age of fifty, it’s closer to one in two hundred. The same test, the same dogs, a completely different statistical landscape.
And that means you need a lot more people to show the result convincingly. If you want to detect, say, a hundred undiagnosed cases of cancer, you’re looking at testing at least twenty thousand people. So we’re running a large prospective study with partners across India where we’ll be testing that number of people, and then comparing that tested group to the current standard of care - showing that the number of cancers detected early through our test is meaningfully more than what’s being currently achieved without it. If we show that, it really means that deploying this on a population level will lead to earlier detection that ideally ends up saving people’s lives.
Two questions on methodology again. The first might be an ignorant one. You mentioned that for these kinds of studies you have partnerships with hospitals for samples, and for the last one you had a lot of volunteers sending you their samples. How does that work? How do you even put this group together?
So we basically have two sets of trials running to achieve this prospective validation.
The first we’re calling First Alert, and it happens in hospitals. We have about eight partners in Karnataka and are onboarding more across India as we speak. Here the participants are people with no history of cancer - essentially people who are already in the hospital for other reasons. Attendants, family members accompanying patients, people there for a regular checkup. We have a kiosk, or we have a couple of our team members there, asking people if they’d like to volunteer a sample and get a report back. It’s a low-friction way to reach people who are already in a clinical setting but aren’t there for cancer - which actually makes them a pretty good proxy for a general screening population.
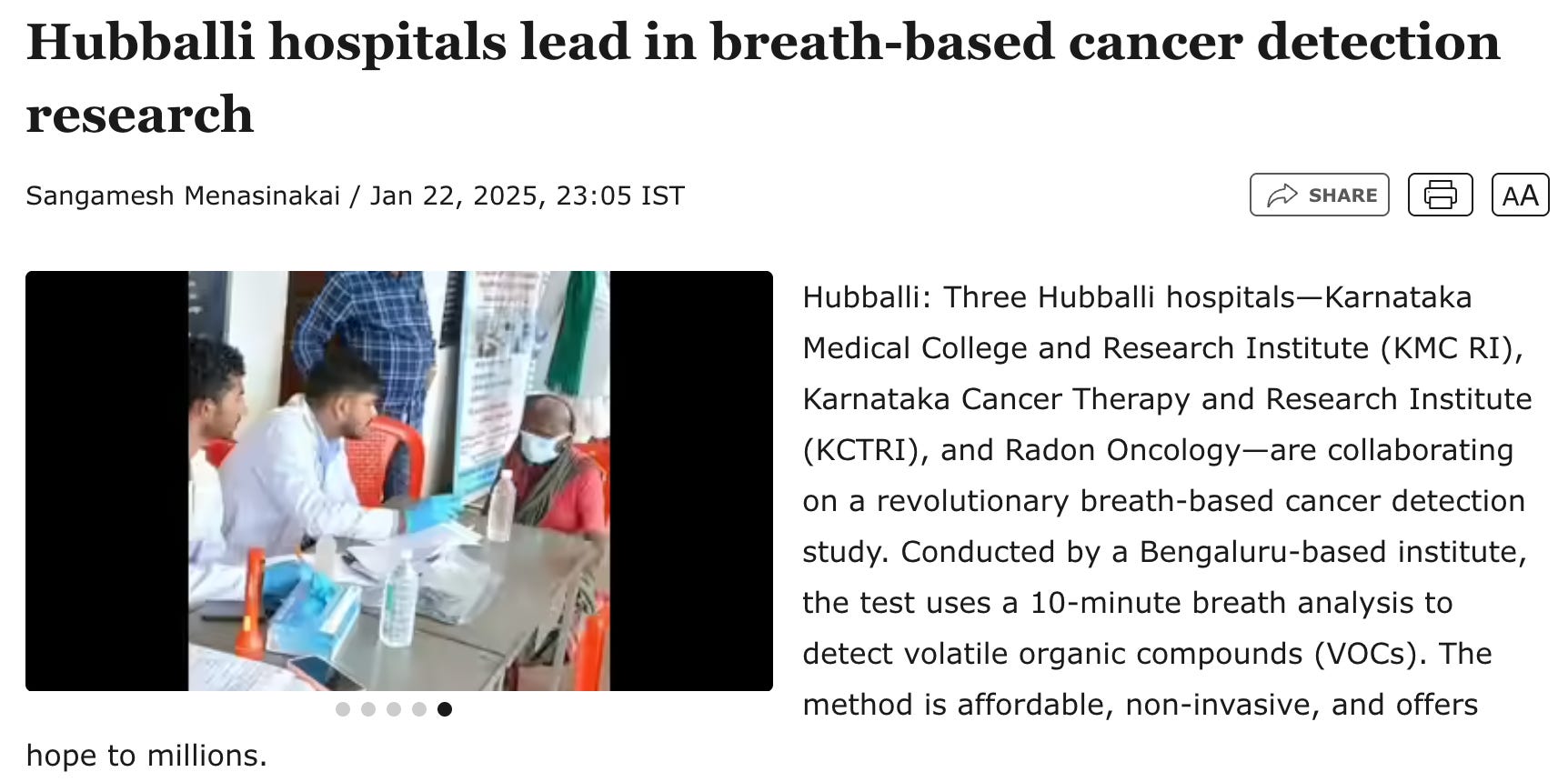
The second trial is called Sanket, and it happens in community health camps - implemented by all kinds of organisations, including the government and NGOs. These camps already run three types of cancer screenings recognised by the government of India, for oral cancer, breast cancer, and cervical cancer. What we’re doing in Sanket is randomising the camps. In half of them, we just track participants and how many cancers are detected by those three standard-of-care screenings. In the other half, we add our breath test on top. Then we compare. About 30,000 participants total, split into 15,000 each.
The goal is to show that with our test, the number of early cases of cancer detected is significantly more than in the camps without it. In other words, we’re not just trying to show that BreathEasy (our mask-based sniff test) finds cancer. We’re trying to show that it finds cancer that the existing system would have missed entirely - cancers that would have gone undetected until symptoms appeared, by which point it’s often too late. If our test downstages population cancer incidence - shifting diagnoses from Stage Three and Four to Stage One and Two - then there’s a huge argument to be made that it should be rolled out everywhere. Because catching it early has enormous implications for treatment, survival, and cost.
Got it. My other ignorant question is around incorrect results. Obviously this is a high stakes exercise. Both a false positive and false negative can be potentially catastrophic generally - and that’s true for any cancer screening test not just yours. What happens in those cases? Are there repercussions for the tester?
It’s definitely one of the trickiest things with cancer screening. Both a false positive and a false negative carry real harm. The false negative gives you false assurance that you’re okay. And then it turns out in the future that you might not have been okay, and it was just missed. The false positive carries the harm of anxiety about having something you don’t actually have. And with something like cancer, that anxiety can be serious and needs to be treated with a lot of gravity.
And you’re right that no screening test can solve for both. It’s always a trade-off. It’s just a fundamental fact about any diagnostic test - you set a threshold somewhere, and based on where you set it, you’re optimising for one at the cost of the other. Set it too sensitive and you catch more cancers but also flag more people who don’t have it. Set it too specific and you miss fewer healthy people but also miss more cancers. There’s no free lunch.
The way you manage this is through communication - how you frame what the test result means and what the follow-up looks like. It’s very important for us, and for any cancer screening test, not to imply that a positive means you have cancer or a negative means you don’t. It’s all about risk. How much risk you might have. So a positive would be conveyed as: you might be at elevated risk, but we don’t know for sure. This does not mean you have cancer right now.
And I know that’s easier said than done, because what does high risk actually mean to someone sitting at home reading a result? We do think in binaries to a certain extent - you either have something or you don’t. But we’re not the first to navigate this. Other tests have done it.
If you look at the mammogram - the false positive rate is about twelve percent and the false negative rate is about fifteen percent, if not more. That’s a lot more than our test. And the prevalence of breast cancer, as compared to multi-cancer, is much lower. So you end up with a lot more false positives. But the mammogram is still rolled out everywhere in developed countries and recommended as standard of care, because we’ve collectively recognised that the benefits of catching cancer early outweigh the harms caused by false positives and false negatives. That recognition didn’t happen overnight. It took decades of evidence, clinical guidelines, and training of both doctors and patients on how to interpret results. We’ll need to do the same work.
We think, given that we’re better than standard of care on those numbers, and given that we’ll be careful with the positioning and communication of our test - with the strong validation we’re seeking to achieve this year - it makes sense to roll this out with the right training in place.
That makes sense. So you mentioned this next milestone - you're running a large prospective study, testing people who don't know if they have cancer and following up on the results. What does that actually look like in practice? When does it start, how long does it take, and what are you hoping to show at the end of it?
The stakes are definitely higher with this study. The previous one was observational - retrospective, as you might call it. The person had already been diagnosed. They were going to be treated regardless. We were just coming into that window, getting their consent and their willingness to contribute a sample. It wasn’t changing their treatment trajectory or anything that materially affected them.
Here we’re stepping into different territory. We’re testing people with no cancer history and then following up with a report within two weeks, working with the clinicians at each site to figure out what the follow-up should be. That means we have a responsibility to those people that we didn’t have in the Phase-2 study. If we tell someone they’re at elevated risk, we have to see that through properly.
We went through a lot of iterations on the protocol and we’re still refining it. But we’ve set up several governance mechanisms. We have what’s called a trial steering committee - an independent body of experts that monitors the study, provides input on the design, does check-ins to make sure things are going as planned, and has the authority to stop the trial if needed. We just got confirmation of a really senior researcher who has led previous large multi-cancer detection trials in the UK to chair this committee. And we’re now assembling other experts - statisticians, community health experts, psycho-oncologists - to provide input on how to carry this out properly.
The follow-up works like this. After a positive result, the person consults with a clinician. If there are already any symptoms, we do a targeted screening based on what those symptoms indicate. If there are no symptoms, we do a PET-CT - the gold standard test for detecting even early stage cancer. The PET-CT is expensive, and it has some radiation exposure. But the alternative - giving someone a positive result and not having a gold standard follow-up - is also ethically fraught. Going with the best possible follow-up was what the chair of the trial steering committee recommended.
After the PET-CT, if it’s positive, the person gets confirmed with a biopsy and starts treatment. If it’s negative, it was a false positive and they’re in the clear.
We’re looking to launch in the next couple of months - starting from June, with implementation partners who already run community camps. We layer on top of what they’re already doing. And then after positives from our test, that’s where we take over, fund everything related to the follow-up, and reach the conclusion by the end of about nine months after enrolling all the people in the trial.
VII. The Business
So all of this progress on the scientific and technological side of things - where does that leave you from a commercial perspective? Obviously it’s still early, but you and Itamar were clear from the start that this would be a commercial venture. You’ve been working with various hospital partners already. Do you see these as pilots or proofs of concept, or are these just open-ended explorations for everyone to learn?
We have two pathways running simultaneously. One is protocol-driven research - the prospective trials we’ve been talking about, which generate the gold standard evidence. The other is a commercial pathway with some hospitals, where we have an agreement to provide our service to any of their clients walking in.

In those commercial agreements, this year we’re providing it subsidised - essentially free, maybe a token amount. We’re not charging anyone yet. These pilots are meant to build validation, build trust, and build our capability of carrying these out at scale.
Next year we’ll convert those into paid contracts. Either the end user pays for it, or the hospital has a partnership with us to distribute our tests. But next year is when we start the real commercial go-to-market.
What does the idealised, commercial go-to-market state look like for Dognosis? Who are your ideal customers? How are you envisioning the model? What are you actually selling? Is it the BreathEasy tests? Is it a service? Have you plotted out what the commercial actuation would look like?
I know this is a commercially-specific, pragmatic question, but I’d like to take a step back and look at the wider frame.
Fifteen thousand years ago, the deal that humans struck with the wolf that became the dog was: in exchange for sharing our resources, you help us sleep well at night. Stay on guard. Protect us from dangers that we can’t really sense but that you can. And in some sense that’s the deal that has stayed true ever since. Dogs provide the security of being watched over, the sense of someone being on guard for us.
And that’s ultimately what we’re also offering. With the technology we’ve built - the ability to translate what the dog is smelling, to give us capabilities we didn’t have before - it’s not just protection from bombs anymore. Now it’s diseases. Because we can know with much more granularity what the dog is smelling. And also the scale. No longer does the dog need to be in the same room to tell you if something is wrong. A dog in Nelamangala can tell a human in Mumbai that they might have an early sign of cancer. That’s the same ancient deal, just running at a completely different resolution and range than anything that was possible before.
The scale and the translation that our technology enables allows us to take what the dogs have always been doing - watching over us - and inflect it into a new paradigm. So the service we’re selling is this: we’ll have a team of dogs watching over your health. Every three months or so you breathe into a face mask, ship it to our lab, we analyse it with the dogs and AI, and give you back a report. If something is off, you get the more expensive confirmatory test. But for most people, most of the time, it’s just the feeling of being able to go to bed at night knowing that most likely there’s nothing wrong.
Two follow ups - one, as you have all these conversations with potential partners (hospitals, state governments etc) - do these conversations tend to still start off with incredulous reactions? Or is that slowly changing? And two, I assume the eventual market construct is B2B2B or B2G2C. My question is whether you have to eventually win over the final customer here as well? Or does that not matter, like if this is the best solution, it’s the best solution, and no one cares who or what is behind it?
Both great questions. In healthcare it’s complex, because yes, there’s the end user - an individual. And there’s the hospital, which isn’t entirely separate from the clinician but in some sense is two different entities. The clinicians are ultimately the endorsers. You have to win their trust if you want to sell a healthcare product.
This is especially true in India, where there’s still a lot of trust and faith in clinicians. In the US you see this eroding - people more and more want to take healthcare into their own hands. In some metropolitan cities in India you see some of that too. But we’re firmly committed to the idea that something as novel and unprecedented as this needs the trust of the healthcare system. You want to work with it rather than against it.
So we see this primarily as a B2B2C model - working with hospital partners, healthcare chains, and diagnostic chains across the country to get this to the end user.
What we’re seeing from clinicians is actually encouraging. A lot of them already know about this. They’ve read the papers about COVID detection, the papers about cancer. They know the dogs have been doing this for a while. Their question has typically been something like - yeah, we never really knew why this didn’t become a thing. It would come up in the news one year and then disappear. And then we explain the thesis of why we think that was the case and how we’re solving for it. We show them our data, the fact that we’re now publishing in the world’s top oncology journal, the gold standard prospective studies we have lined up. We’re giving them the steps they need to build trust in the product. The reception has been good.
The challenge in India is that we simply don’t have a mature cancer screening market or product category. Less than one percent of Indians are screened in their lifetime. In the US, the mammogram is basically a regular visit for most women. That’s simply not the case here. So there’s a behaviour shift we’re asking people to make, which is always harder than selling into an existing habit. We think having something that’s easy, that can be done at home, with none of the friction or cost of current methods, changes things radically. But we know it’s still somewhat of an uphill battle with an early detection product in India. The US is a market we’re also actively pursuing, where that screening habit already exists and where the willingness to pay for preventive health is much higher.
But what we’ve realised in the last three months from the oncologists we’re working with is that they care just as much - if not more - about something else entirely. Not just detecting cancer in an undiagnosed individual, but detecting the recurrence of cancer in a cancer survivor. Because cancer can and often does come back. If you treat someone for cancer, it’s not always a one and done situation.
And what we found is that the same dogs, in the same system, can detect cancer coming back with the same accuracy they detect it the first time. It’s the same signal. We’re building a larger dataset for this, but in the pilot we ran, the results held. That’s actually a significant finding, because recurrence monitoring is a problem that even the most advanced oncology centres in the world haven’t fully solved. You treat someone, you send them home, and then you’re largely dependent on follow-up scans and symptom reporting to catch a recurrence. Our system could change that.
Oncologists are already really interested. When they treat a patient, they want to know that patient stays healthy. It’s a personal investment - oncologists know almost all their patients by name, they’re really invested in the journey. And they always have in the back of their mind: what if it comes back? If it does, can we know soon enough to still have a fighting chance? And patients are on guard too. That feeling of anxiety never fully goes away after a cancer diagnosis. The feeling of being at ease that we can offer is even more pronounced in that context.
So in India we have a two-product strategy - launching early detection and recurrence monitoring simultaneously. Early detection will find traction with people already invested in their health, doing full body MRIs and full blood checkups. Recurrence monitoring fills a gap that is enormous in India, where we just don’t have alternatives at an affordable price point.
And what about the final perception of consumers - is that something you think about alot? Is that something you need to think about alot?
Yeah in a funny way it’s actually been a positive by-product of what we’re doing. Dognosis naturally evokes curiosity and a desire to understand and know more and even participate in what’s happening here. When otherwise someone would not be interested at all in getting a colonoscopy. I mean, can you blame them? It’s not exactly a fun activity.
But breathing into a mask and knowing it’s being analysed by a team of dogs and AI is actually appealing to people, strange as it seems. We’ve seen adoption because of the way it’s done, not in spite of it. And that’s something we want to lean into rather than shy away from. There is a model where the person doesn’t need to know how the test is being conducted. But in that model, we probably wouldn’t be called Dognosis.
What about governments here, and specifically the Indian government. What do these officials think of Dognosis? What are some of those conversations like, about working together closely now or in the future?
We really do think that what we’ve built, and what the dogs are capable of, and the modality of breath - which doesn’t require infrastructure or cold chain or any of the things that make implementation really hard - is genuinely well suited to public health, both in India and across the world. These aren’t nice-to-haves. They really determine whether someone gets treatment or not. Breathing into a mask and shipping it over, with a team of dogs that can be maintained at pretty low cost without breaking down or requiring specialised labour to operate - it’s a natural fit for the problem.
But public health, both in India and elsewhere, is built on decades of evidence generated through large randomised controlled trials. That’s just the reality of how the system works. Before you roll something out to the public, stakeholders want to see it really battle-tested. WHO endorses it, or ICMR endorses it at the national level. Policy has to change. You have to win a lot of people over. These things take time. And that’s not necessarily bureaucratic obstruction - that’s actually the right standard. You don’t want population-level health interventions rolling out without that level of scrutiny. We just have to work within that reality.
We’re launching our large randomised controlled trial both to generate evidence for this specific application and to establish the efficacy of the test more broadly. We really want to see this work in a public health setting, and we’re very open to working within the cost constraints of what government implementation would look like - once the validation is there.
But we’re also realistic that those timelines are longer than what can sustain a startup. So our focus is the private channels, while keeping the door open for the public pathway when the time is right.
How do you see the competitive environment? Who are you competing with, and why does Dognosis win in the long term?
First of all, I think the competition is the status quo. The status quo is people that are detected late, and despite us having treatments that could have saved them if it was detected early, they unfortunately pass away. The other status quo is the fact that capital and the market has decided that the solution to spend the most money on is extremely expensive immunotherapies and chemotherapies. Which are important - we want cures for cancers. But a lot of times the cure can be just detecting early. So the status quo is probably our biggest competition. There is enough cancer to be detected that a lot of other companies can be in this space and it’s win-win.
In terms of specific approaches, there are basically three broad categories - the animals, the centaurs, and the machines. Companies working with biological sensors alone, companies working with bio-hybrid systems that fuse biology with AI, and companies trying to do this purely with machines and e-noses. Dognosis is in the centaur model - fusing what the dog can do with what AI can do.
There are a few other companies trying to build something similar. Two Israeli companies - one working with dogs, one working with rats. Both have an AI component and a thesis on how it helps solve the problems that have historically prevented biosensors from working at scale. Those are the companies we watch most closely, because they’re attacking the same fundamental problem from a similar angle. We’re neck and neck with them, but we think our technology is better suited to playing to the dog’s strengths than theirs, but they’re the closest competitors. They’ve done similar validation studies, they’re exploring US go-to-market, they’re building up evidence.
Then there are companies taking olfactory receptors from insects or mice and embedding them on chips connected to neural networks - taking the organism out of the picture entirely and just keeping the receptors.
There’s a company in New Zealand doing this, a couple in the US as well. And then the pure machine e-nose companies, which still face the same fundamental problem that biological sensors are just more sensitive. They have workarounds, but the resolution gap remains.
I’d say it’s still early enough that no one really has a clear edge. Some are better funded than others. But it’s not clear who’s going to be the winner. What is clear is that the olfactory detection space is real, it’s moving, and the question is no longer whether this can work - the dogs have answered that. The question is who builds the system that makes it scalable.
Could you touch on the scaling point where it pertains to Dognosis too? Is it possible to scale the current approach to handle a meaningful number of tests in a given population? And if the dogs are always going to be in the loop, does that mean you’re always constrained by how many tests a single dog or pack of dogs can do in a day or month or year?
Our estimation is that a team of 30 dogs could do one million screenings in a year. A million tests is a lot of tests. It’s the same number that BillionToOne did in the eight years from being in YC in 2017 to going public on the Nasdaq in October 2025. They did a million cumulative tests and then went public. So if we do a million tests, you’re probably at the stage of being a public company - because you’ve created a lot of value if those tests are meaningful, which detecting cancer is. Even with 30 dogs, being able to reach that milestone feels like it unlocks a real level of scale.
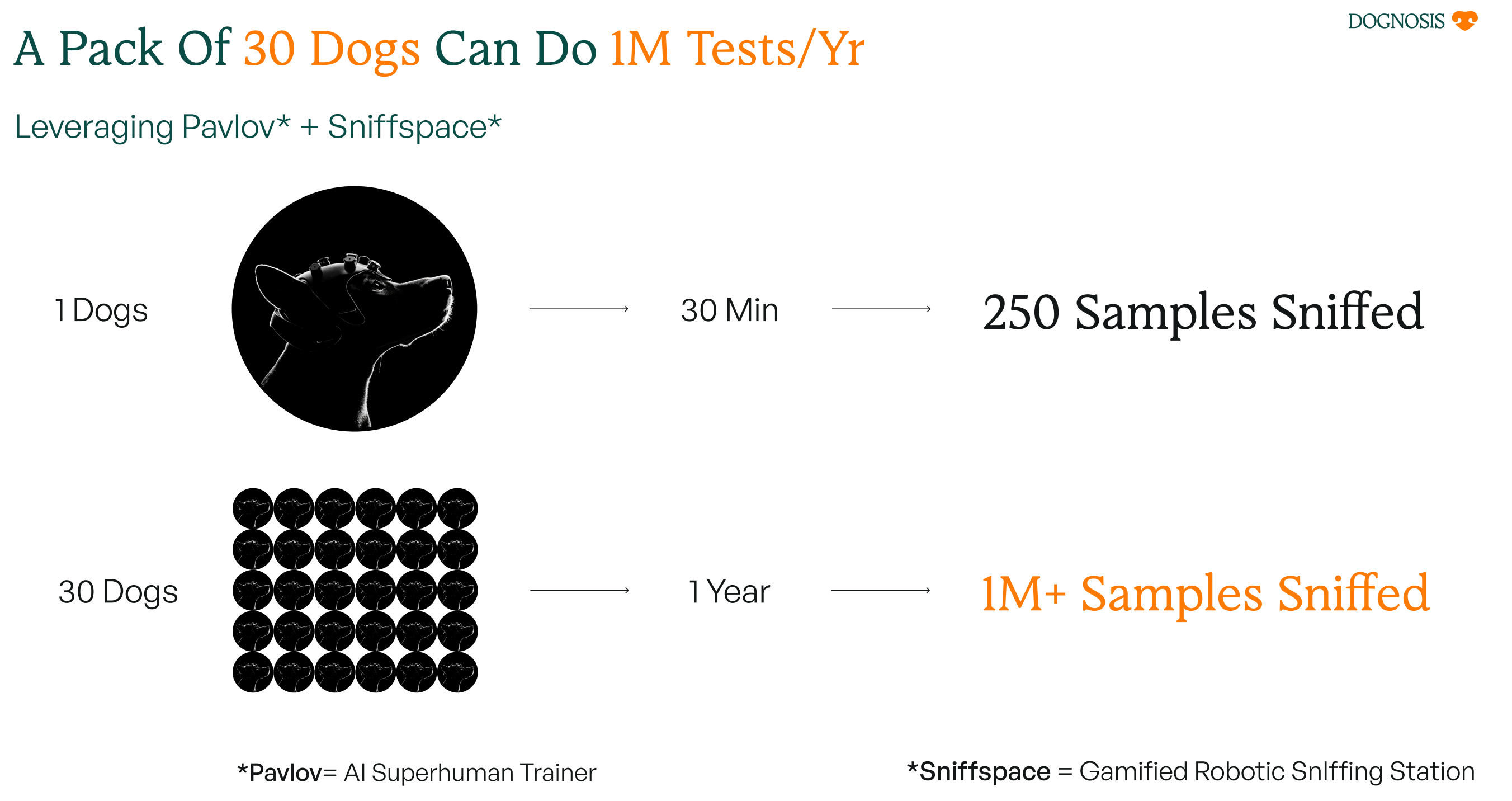
I wouldn’t underestimate just our Bangalore centre being sufficient to really change how we think about medicine. But if you’re thinking about screening the entire population of the world - for cancer you basically want to screen everyone above the age of forty, something like three to four billion people - that’s a lot more than a million.
And I don’t see a good reason why the dog model isn’t scalable. There’s no shortage of dogs. There are more dogs than children in the United States, and it’s true of many other countries too. And you don’t need very special dogs to do this once you’ve built the technology to read them. You need special dogs only if you need them to give special responses. We don’t. The selection criteria is just a passion for sniffing and a passion for food, which we talked about earlier.
There are a lot of different models that could make sense in this future - sniff gyms, setups embedded in hospitals, neighbourhood diagnostic centres. Different ways to democratise this kind of olfactory inference at scale.


And there’s something else worth saying. Dogs deserve a life that has purpose and cognitive enrichment. Dogs have worked alongside humans to do exactly this kind of thing right from the start of our mutual friendship. It’s only in the last thirty years that humanity has essentially said to dogs - sit at home in a small apartment and I’ll occasionally take you for a walk and that’s your life. All our dogs are genuinely happy to sniff on the platform. It’s fun for them. It’s what they’ve evolved to do. So I see this as a real win-win. And at least for the next five to seven years, a couple of centres gets us a very long way.
Are there arguments against Dognosis or your approach that you think are reasonable? Are there people within the traditional medical or scientific communities that vehemently disagree with your approach?
The idea that dogs could ever be part of medical infrastructure - the reception to that varies a lot depending on where you are. In India, a lot more clinicians are open to it because they see the starkness of current screening and how resource constrained it is. They know the problem is real and they’re not precious about what the solution looks like.
When we’ve talked to clinicians and researchers in the UK and the US, there’s generally been an acknowledgement of the science. But then there’s a dismissal that’s almost an optics or perception piece. Something like: no, dogs can’t be the future. The future has to be a fancy sequencing machine or an MRI. Some people just won’t buy into canine olfaction being an important piece of medical infrastructure, full stop.

But when it comes to the core thesis - that we still haven’t solved for that first layer of cancer screening, that if you don’t solve the population-level needle in a haystack problem first, no test is going to work at scale - we see a lot more agreement there. The criticism of current cancer screening that Mukherjee laid out in The New Yorker, the problems with the Bayes Law (statistical) issue at population level - that resonates with everyone working in oncology. They know the problem. What they haven’t fully seen yet is that breath and dogs can solve for that first layer, and that liquid biopsies then do the second. The breath and blood one-two punch. We think the thesis is just underrated and under the radar right now. But the feedback we’re getting from people who engage with it seriously is that it does make a lot of sense.
In terms of arguments against our specific approach that I think have some merit - the strongest one is the question of why use the whole dog at all. Just take the olfactory receptors, put them on a chip, connect them to a neural network, and you have something without the messiness of a living organism. On paper it sounds logical. And honestly, at Dognosis we think that might where things end up eventually - what we’re doing could actually lead to that. It’s a question of timing. We know the dogs can detect cancer. That’s technically de-risked. It makes more sense to have the interfacing layer delivering value to people while the R&D on the receptor question happens on the side, rather than betting everything on solving both simultaneously. But the argument is a reasonable one.
The other one I see some merit in is the scaling question. With our centre in Bangalore we can do a million tests a year, and that’s a lot of tests - more than most diagnostic companies have done at this stage. So we don’t see challenges with scale in the next five to seven years. But if you’re talking about screening a billion people, there are ways to solve it, but they’re not trivial. That’s a legitimate question.
For the most part though - there’s got to be a company that wins in the olfactory space. And we just have no good reasons why that company isn’t Dognosis.
Mouse-nosis doesn’t have a good a ring to it anyway. So I think you guys have got the perception lead on that front as well.
Yeah, I think we have the best name out of all the companies in this space. No doubt. Indisputable.
IX. The Future
What does the the world of 2035 look like to you? How do you see the future of medicine? Do you think our relationship with diseases or our approach to tackling them will look a lot different than it does now?
There’s a lot of talk about moving from a reactive to a proactive healthcare system. Healthcare is ‘sick care’ right now, but it doesn’t have to be. Everyone’s in agreement on that, it’s almost become a cliche.
But even if you get the incentives right - as you guys wrote about in your piece on Even, that’s still actually really hard to do - we currently don’t have the tools to enable a genuinely proactive system. Like, we have vaccines for some diseases but not all. And the future of disease increasingly looks like non-communicable lifestyle diseases, cancers, heart disease, neurodegenerative disorders. For most of these, we don’t have screenings. We don’t have a way to catch them early and intervene before they become full-blown and really hard to treat.
Leave aside the Brian Johnsons of the world who can throw everything at the problem and maybe come out victorious. What about the rest of the world? How do you actually change healthcare as a whole, even if you get the incentives right?
We think you need a platform and technology that unlocks the democratisation of preventive healthcare by becoming an early warning sentinel system. Someone watching over you, on guard, catching diseases as soon as they appear. This is exactly the agreement we’ve always had with dogs - watching over us in exchange for being part of the pack. What’s changed is the scale and the precision with which we can now act on what they’re telling us. And I really think there’s nothing stopping this vision - Dognosis as a breath-based screening network powered by canine olfaction - from being the solution for multiple types of diseases, starting with cancers but then moving on to others, where we truly can detect disease at its earliest stage and have treatments designed to cure or prevent it from developing further.
That just changes the whole paradigm of how we think about healthcare. Right now all the resources and capital go into the latter part, into treatment. But once you shift the curve earlier, you see a completely new picture of what healthcare can look like. And the numbers are stark - in India alone, a million people a year could be saved if cancer was simply detected earlier. Not with new drugs, not with new treatments, just earlier detection of what’s already there. And this frontier of human health, of living longer and better, isn’t just restricted to the few people who have millions of dollars to throw at the problem. It’s accessible to everyone.
For this future of medicine - what are the milestones we need to see to get there? And how do you see Dognosis’ role in this future too? Where are you embedded in the value chain of public health, in India or abroad?
I think the role of Dognosis is to provide the olfactory inference infrastructure to enable breath-based screening. But that’s not the whole picture. This is really an alliance, of hospital providers, insurance companies, therapeutics and pharma companies. Dognosis is one layer of that. We think that layer has a lot of leverage because it changes the distribution of illness at a population scale. But it’s definitely not the whole picture on its own.
By building this infrastructure, we hope to essentially create an API-to-the-dog-superpower to anyone who needs it. So it can be public health groups around the world, healthcare providers serving private users, or just the individual and the family who can avail this service directly.

I think the milestones getting there are, first, this next year of proving that our system can work in the real world - detecting undiagnosed cases. That first case, when we get a sample from someone, find an early stage cancer, confirm it with a biopsy, start them on curative treatment, and they continue to do well. That moment is going to be a huge inflection point. This is no longer something you read about in a press article. It changed someone’s life materially. That’s the first big milestone.
The next milestone is showing this system can be sustainable at scale - screening people across metropolitan cities in India, figuring out the operational challenges, maintaining high quality controls and accuracy, and doing this sustainably. We prove that we are providing value and can be on our own paws going forward.
And then it's just a series of building the next steps. I think the moment when we’re able to actually prove that a dog can walk onto a platform, suit up Iron Man style - the helmet and the harness go on - run a whole session testing five hundred people, basically screening a village in half an hour, and then walk out without a human needing to be in the room at all. The next dog comes on.

Once we reach that stage, which we expect to this year, what is stopping that from replicating across the world? You set up a platform, find your pack of dogs, get them trained, and they’re screening villages every day. That’s when this stops being a startup and starts being infrastructure.
There are going to be challenges - regulatory, operational, commercial. But those three milestones, finding that first person and changing their life meaningfully, achieving fully autonomous sessions, and building a sustainable initial go-to-market - once we get there, the momentum is on our side.
You said those three things - regulatory, commercial and operational. If Dognosis doesn’t work, or doesn’t pan out the way you think it would be, would those be the reasons? If we did a pre-mortem today on why this might not work, what reasons would we find?
There are a few good ones. The first is the regulatory grey area around how a system like ours gets classified. A lot of it hinges on whether the jurisdiction has a framework for Lab Developed Tests, or LDTs, where you don’t regulate a device but a laboratory process. India actually doesn’t have an LDT framework in law, but in practice one exists through the NABL, which aggregates labs. But there’s still grey area - is a dog sniffing a sample a lab developed test, is it a medical device, is it something else entirely? We’re working with regulators and have an experienced team member helping us navigate how first-in-class systems like this should be classified. But no one has really done this before, so we’re all treading on new ground.
There’s also still an open question on whether we’ll be able to provide this in the full capacity the technology allows, or whether we’d have to tie our hands and provide something that doesn’t deliver the kind of value we’re hoping to deliver. We’re optimistic. But it’s a question mark we haven’t fully solved, especially in the US where it’s an active work in progress.
The other piece, if things go wrong, is losing trust. If we rush to market without fully validating and getting clinicians to support this, and then inevitably hit the real trade-offs of any diagnostic test - imperfect sensitivity, imperfect specificity, false positives and false negatives - without the foundation of trust in place, I can see things turning against this approach quite quickly. The N-Nose situation in Japan is a useful cautionary tale here - they scaled direct to consumer before the clinical evidence was solid enough, got criticised by Nature, and now struggle to be taken seriously despite having run nearly a million tests. That’s why it’s so important not to rush into the commercial story before building out the gold standard validation first. Once you lose trust, it’s really hard to get it back.
On the positive side, you’ve just raised a round of seed funding from Accel Atoms. That’s come at the end of a long fundraising grind for your seed round. For an idea like yours, I can imagine that it’s easier for investors to find the ‘no’ than the ‘yes’. What have you learned about fundraising over the last few months that you can share, especially advice that may help other founders similarly working on groundbreaking ideas that aren’t immediately legible to an uninitiated audience?
Well there were a lot of no’s. We spoke to over a hundred VCs, it’s been mostly no’s and just a handful of yes’s. We were lucky early on to find investors like Boost VC and 1517 Fund who backed us because our idea was audacious and our ambition was unbounded but also grounded. They really carried us through that initial period - two and a half years of Dognosis now, though it’s hard to believe when you’re inside it.
But when we had to raise the seed round - a larger round to take us through the next set of pilots, trials, and technology validation, with no revenue on the horizon until next year - the stakes were higher and it was a real grind.
Part of it is that cancer screening and diagnostics has traditionally been underfunded. That’s just the domain. But the bigger challenge was that Dognosis is simply not legible to the current trends in AI and hardware that investors have built theses around. No one is thinking about biological sensors and intelligence as something that current models and technologies can’t replicate, and that we can translate those capabilities to solve problems that have long been unsolved. That’s the thesis. It’s a real thesis. But nobody had it sitting in a deck waiting for us to walk in.

So a good chunk of the no’s came from people unwilling to believe dogs could scale or that the idea made any sense at all. Another section struggled to figure out how we’d actually go to market. And underneath those doubts was probably also a question about Itamar and me - backgrounds in cognitive science and canine science, building a company that ultimately needs to integrate with healthcare systems and become profitable - whether we could really pull that off.
Which I find interesting, because until now the challenges of actually making this work in the first place have felt a lot harder than the commercial challenges coming up. Which are not trivial. But once you have a system that can detect cancer from breath, at a price point way cheaper than anything on the market, with sensitivities way better than anything on the market, and a user interface that is simply breathing into a face mask at home - selling that product feels a lot easier than getting to this point of building it.
Not everyone is going to be convinced. But those who mattered, we were able to convince that we were serious, that this was a life project, that we had made real progress, and that even though it felt implausible, this idea is really inevitable. It’s been in the making for a while. We are the people to make it happen.
If you have an idea that’s illegible, you have work to do to make it legible. And then you have work to do to prove you’re the founders capable of making the jump. Ultimately, all the people who backed us backed us as founders and as a team. And that was the most key piece.
X. Closing
You once wrote a blogpost that I really loved. You said that Dognosis is the ‘hardest, easiest, and best company to build’. Do you still believe all three things?
I think I wrote that just one day when we had a really hectic and tough week, where everything seemed to be breaking at the same time.
I started with why Dognosis is the hardest company to build. Because we’re doing something that people think is crazy - science fiction or pseudoscience. We’re doing it in a really entrenched industry, cancer is the largest industry in healthcare, with incumbents who have been doing this for a while and have every interest in preserving the status quo. And you’re doing it as the underdog, with this approach that requires stacking five different systems that all have to be built in house.
You need to build clinical operations from scratch, because breath collection is a novel modality that doesn’t exist yet. You have to train the dogs yourself, that’s not something you can outsource, it’s a core part of the system. You need to build novel hardware to read and write to the dog. You need the software to make that hardware work. And then on top of all of that, you’re building machine learning models to do it all autonomously. Each system has its own domain, all of them have to interact and work together, none of them work without the others, and all of them have to happen at the same time. It’s a crazy concoction. It feels like chaos every single day.
But at the same time, because of what we’re trying to do and the audaciousness of the goal and just how mission-aligned with doing good it is - it’s really asking the question, we have this incredible capability, how do we unlock it so it can do the most good? How do we detect the most cancer as early as possible? And that’s pretty cool when you think about it.
Because of that, you can attract incredible people who are also excited to work with dogs. Every time I tell people what we do, people are willing to listen. They have a reaction. It doesn’t just go, oh okay cool. Anyone can connect with what we’re doing. People know someone in the family who had a fatal brush with cancer. They’re dog lovers. Something about it is just so relatable and so interesting that a lot of rooms and doors open just because people hear what we do and they’re excited. So it’s also an easy company to build in that sense, where you’re perpetually motivated.

And it’s the best company because who else gets to say that you go to this farm in the outskirts of Bangalore, working with tech and doing frontier research that is hopefully doing good in the world, and you do it with dogs, who I’ve always loved. I had this childhood dream of living on a farm with tens of dogs. That’s kind of come true. I couldn’t have asked for anything else.

Last couple. One is, what have you learned about dogs since you started doing this? What have you learned that you didn’t know before? What has surprised you?
The first time I heard about all this, it was just an abstraction, right? Dogs can detect cancer, dogs can detect COVID, all with this remarkable accuracy. I got obsessed with trying to understand how they do it. And then as you dig into it, you just realise there’s all this other stuff that still remains unanswered.
We still don’t have an idea what molecules they are detecting. That’s crazy to me. There’s another thing I learned recently - dogs have a heat sensor on their nose which can actually measure warm and cold as well. That’s why their noses are always cold and damp. They have this whole other sense that I didn’t even realise till a couple of years ago. There’s probably so much more that we still don’t know, right?

So you have these complex biological beings, but everything they’re doing just looks and seems so simple. The thing is I’ve always loved dogs. I think my earliest memories were with dogs. And I’ve never really had an impulse to feel like I fully need to understand them, because they’re just obviously different beings. You have no idea what their world looks like, what their experience of every day is. But what I appreciate so much more now compared to when I was growing up is the juxtaposition between their simplicity and complexity. On one hand, this dog will sniff a mask and instantly make a decision about whether it contains the faint traces of a life-threatening disease. And then as soon as you go into the yard, this same dog will jump on you and roll on the ground with you, and sometimes eat its own poop. I just find them fascinating.
And then there’s this other thing that still surprises me - the connection. One of our dogs, Snow, me and her have this great friendship where she’s the only one I can completely let off leash when we’re walking around the farmland, because she always comes back. And I just think about that sometimes. This other being that they doesn’t speak our language, have a completely different intelligence and perception of the world - how do they connect with us in this way? How have we established this relationship that allows for doing what we’re doing right now? I genuinely have no idea. But I’m glad we do.
Tell me more about Snow - she’s come up a few times and seems to play the role of OG on the team. And do you ascribe strong personalities to other four-legged members of the team too?
Yeah she’s one of our OG beagles - the oldest on the team, about four and a half, five years old, though we don’t know her exact age because when we adopted her we only got a general sense of it. She’s actually the mother of some of our other beagles, or at least we think so - the family resemblance is hard to miss.
Snow was originally recruited as a cancer sniffer. She didn’t work out. The problem was that she lied. A lot. She would indicate cancer on samples that didn’t have it - and you could tell that she knew, she just thought: why not give it a shot? That tendency never really went away. So she’s the only dog on our team who doesn’t sniff cancer.
But she became one of our most important team members anyway. She’s sweet, calm, completely unbothered by new things, and will happily submit to any experiment as long as treats and pets are forthcoming. Which made her our perfect alpha tester - the dog who wore every weird prototype helmet, tried every new harness iteration, and sat patiently through hours of baseline EEG recording while we figured out what we were doing.

She also ended up leading one of our most interesting projects. We won a $75,000 contract with Singapore’s Home Team Science and Technology Agency - their homeland security R&D arm - to solve a challenge they’d put out: could you create a 3D map of a post-explosive scene, identifying where the residues of the explosive used were present across a field? The idea was to have a dog wearing our DogSense smart suit sniff the field, and then use the EEG and respiration data to predict, in real time, where on that field the dog was detecting explosive residues - projected onto a 3D map. Snow ran that project. It turns out detecting explosives is a little easier than detecting cancer, so her lying tendencies didn’t get in the way. She was brilliant.
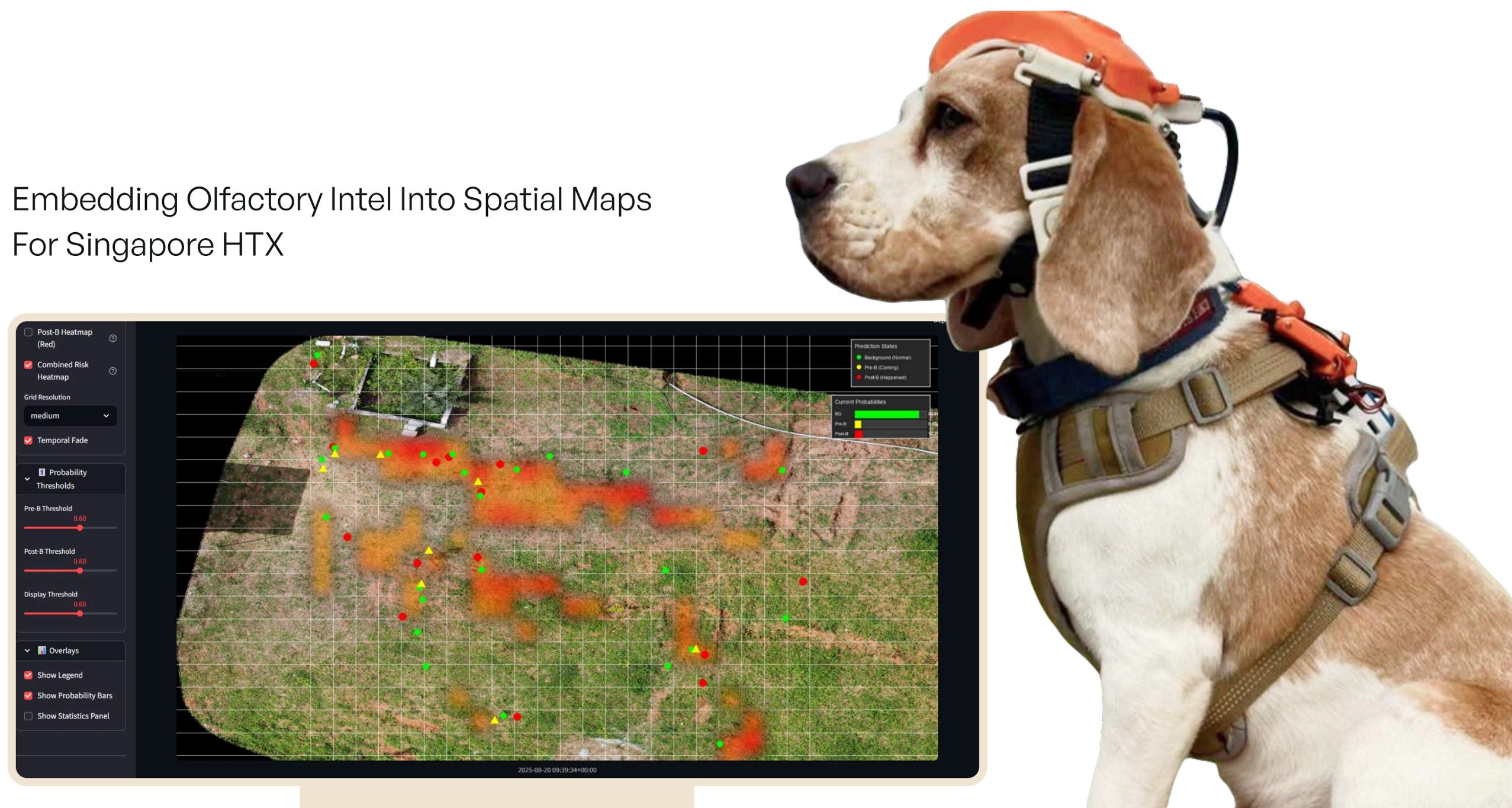
It’s actually a good illustration of something bigger. The technology we’re building isn’t just for cancer. Any domain where dogs are currently deployed - explosives, narcotics, disease - our smart suit can amplify what they’re doing, make it readable, mappable, scalable. It’s like a better interface for K9 units wherever they are, almost like a thought translator for dogs.

Snow is also a good illustration of something else we’ve learned - that dog personalities manifest directly in working styles in ways that are genuinely scientifically interesting. More optimistic dogs tend to have higher sensitivity - they’ll flag more positives, sometimes too many. More pessimistic dogs tend to have higher specificity they’re more cautious, more precise. Scientific American actually covered this recently.
On our team, Banu is more pessimistic - stable, high drive, rarely wrong. Billy is more optimistic - enthusiastic, occasionally unpredictable. We’ve learned to play to their strengths, and our Bayesian (re: statistical) model does the rest - aggregating across the pack to stabilise the wisdom of the group.

This is probably a question I should have asked earlier, because it’s a question I imagine lots of people have when they hear about what you’re doing. But for any people (or dogs) still reading, what does a day in the life of a dog at Dognosis look like? The first time I visited I remember telling you that it seemed like dog heaven, like if I was a dog I’d work hard just to find my way into Dognosis.
We’re in a much better place now (not philosophically but literally). We escaped Bommasandra in the first six to eight months and found this beautiful spot in the outskirts of Bangalore. It’s two acres of what used to be a pomegranate farm, with a farmhouse and a pool. Last time you were here the pool wasn’t equipped with a filter - post the seed raise we decided that was an important investment.
So there’s a farmhouse and a pool and we built these kennel units with big yards and grassy fields. The dogs are taken care of by a caretaker team that lives on site in the farmhouse - four people are there all the time. They take them for walks both in the morning and evening in this kind of farmland, idyllic hill region where there's also a lake. Sunrise and sunset walks are part of the everyday routine, and then a lot of time just chilling and playing in the yard. The dogs all live together and sleep together.
Dogs are pack animals, right? A few dogs prefer to be on their own but most really like being around other dogs - which is something modern dogs don’t really get to do as much. In the west you have dog parks. In India, dog parks are few and far between. Most dogs don’t really meet other dogs or play with them as much as they should. Our dogs get plenty of that during yard time.
And then for about thirty minutes to an hour every day they go in and do a session where they play the game of finding the target odour, where they get rewarded with treats every time they do. And all of them are super excited for that training session, because it’s cognitively enriching - they’re doing what they’ve evolved to do best, which is follow their nose.

And the work itself matters more than people might expect. Dogs aren’t just happier when they have a job - they’re actually better at it. The cognitive engagement of scent work, the routine, the reward - it keeps them sharp in a way that sitting in an apartment simply doesn’t.
So that’s kind of what it looks like now. We’re constantly scheming on more things we can do - creating a dog amusement park is honestly on the roadmap.

And ultimately, the dogs living happy healthy lives is directly correlated with them performing their best, just like humans work best when they’re happy and living good lives. We feel like we’ll only do good if our dogs live well. And we’re directly incentivised to make sure that’s the case.
Last one. You told me at the start of this that you come from a family of doctors. And you didn’t think that that would be a path you would follow. And obviously, you found this incredible roundabout route into medicine and healthcare. What would you say motivates you today? Why is this mission important to you?
Initially, when the idea first hit me (and the phrase is deliberate, it really did hit me), I didn’t feel like I really had a choice in being hit or not. I didn’t have a choice in becoming obsessed. Ever since then, there’s been this kind of growing and mounting suspicion that this is a life project. In its entirety, this quest of Dognosis and detecting cancer is something that I can see myself devoting the next decade of my life to.
There’s just so much more to unpack. Dognosis is both dogs detecting disease, but it’s also dogs and symbiosis, right? And this human-canine relationship, and what we can learn from it. And I feel so certain that this timeline, this life, this is what I’m meant to do.
And so the idea of whether I’m motivated to do what is meant to be my life’s work isn’t even a question. I can’t think of doing anything else. It’s also a case of nominative determinism. My blog is called DogLuk. Dog-Look. That’s my last name backwards. DogLuk. Kulgod.

And so looking at dogs is kind of written in my name. So I didn’t really have a choice on whether or not to do this. The path had already been set for me.
Okay, I don’t think we can top that. Thank you for the time Akash. This was awesome.
More reading/watching/listening
The Catch in Catching Cancer Early by Siddhartha Mukherjea
How to Upend Cancer Screening by Eric Topol
Cancer blood tests are everywhere — here’s why you should be cautious (Nature)
Akash’s Substack (AKA Runs and tumbles)
Akash’s blog (AKA Dogluk)
Dognosis’ Substack (AKA Noseprint by Dognosis)
Akash Kulgod | Teaching AI the Scent of Cancer
Co-founder Dynamics and Early Teams
Towards A 4E Approach To Canine Olfaction
The PROUST hypothesis: the embodiment of olfactory cognition by Lucia F. Jacobs
Akash Kulgod UC Berkeley Cognitive Science 2022 commencement speech
Pessimistic Dogs Are Better at Smelling Cancer—And Other Keys to Disease-Sniffing Success
turning 25 by Akash Kulgod
The Leapfrogging Moment For Indian Healthcare
Dogyssey : Chapter 1 by Akash Kulgod
Dogluk by Akash Kulgod (EV 2022)
Dogs as deep-est tech by Akash Kulgod
Uncannis Familiaris by Akash Kulgod
Dognosis Origin Story by Akash Kulgod and Itamar Bitan
Canine Medical Intuitives by Akash Kulgod
brain reading and writing by Akash Kulgod
As always, if you made it all the way here and you thought this was a good use of your time, it would mean a lot to us if you took a couple of seconds to share this post.

One of the best stories of the last year and more!
Dognosis is one of the most interesting companies rn (straight out of a movie fr). This is a very timely piece!