
Getting Even
A Spotlight on...ransom notes, colonial repair shops, The Innovator's Dilemma, and an Indian startup fixing to remove luck from the business of staying alive



Hey folks👋
Long time no see! A happy (relatively) new year, and a warm welcome to the 2972 new Tigerfeathers subscribers who’ve joined since our year-end piece (the official one and the unofficial one).
We’ve got an epic line up in store for 2026, starting with today’s edition. So if someone sent you a link to this newsletter and this is the first time you’re discovering our stuff, subscribe below to make sure you don’t miss the next one.
Also, if someone sent you a link to this newsletter and you just noticed how long this piece is, we’d like to offer an apology on their behalf - it’s kind of the vibe here🤷♂️
Tigerfeathers is presented by…Dhan

India’s capital markets have spent the better part of a decade playing catch-up with the sophistication of the people using them. Most trading platforms either chased first-time speculators with gamified interfaces, or served institutional clients with tools inaccessible to the serious retail investor. Raise Financial Services was founded to fix that — and in the five years since, it has become one of India’s most celebrated fintech success stories: a profitable, product-first challenger that in October 2025 closed a $120M Series B led by Hornbill Capital, with participation from BEENEXT and Japan’s MUFG.
Their flagship product, Dhan, builds for experienced traders who need speed and precision, and thoughtful long-term investors focused on compounding wealth. That means advanced charting with TradingView integration, lightning-fast execution via a proprietary trading engine, and real-time portfolio analytics designed to help users make better decisions. Over 10 lakh traders and investors use the platform today.
Raise’s ambitions haven’t stopped at the trading terminal. Their ecosystem now spans Upsurge, a financial education platform; ScanX, a markets research and screener tool; and Filter Coffee, a bite-sized media product for the next generation of Indian investors.
The newest addition is Fuzz — an AI research assistant purpose-built for India’s financial landscape. Unlike generic AI tools trained to summarise, Fuzz is built to verify, backing every answer with traceable public sources. It runs on Artham, Raise’s own 7-billion parameter small language model trained exclusively on Indian capital markets data — the first of its kind, and notable enough to be spotlighted at AWS re:Invent 2025.
If you’re looking to level up your investing toolset, consider joining the Dhan community here, or check out the platform below:
And if you’re interested in sponsoring a future edition of Tigerfeathers, hit us up on Twitter/LinkedIn or by replying to this email. With that, let’s get to it.

If you’re in a hurry, and you’re looking for four generally applicable lessons to take away from today’s essay, they would be -
To shoot your shot.
To follow your curiosity, and follow it all the way.
To treat the Internet as a serendipity machine.
To design healthcare systems in a way that align the incentives of the entity delivering the care and the entity paying for it, so the most profitable outcome for the system is also the best outcome for the patient at the centre of it, and everyone makes more money by keeping you healthy than treating you when you’re sick.
Super generally applicable, just like we intended.
That being said, if tidy summaries aren’t your thing, and you’re down to follow us into the weeds, allow us a few paragraphs to give you the backstory on both the author and subject of this week’s Spotlight edition. Given that the actual essay veers dangerously close to book-length, you can treat this introduction as more of a prologue than a preamble (which means both are longer than you’d prefer them to be😬).
Anyway, strap in. We’ll kick things off in September 2025.
Rewind
On the 10th of September last year, The Ken announced the second iteration of its annual case study competition.

Describing the 2025 edition as more of a “case build” competition (*hipster attribute intensifies*) compared to the year prior, the company again invited college students from across the country to pick a real-world incumbent - any company, any sector, anywhere - and design a plan to disrupt it using AI. They upped the ante by challenging students to go beyond the slide deck to build working prototypes, landing pages and functional products to demo their solutions. The winning team could expect a cash prize of INR 10 lakh.
1,084 teams from 127 colleges across the country ultimately sent in a submission. After several rounds of evaluation, a hundred made it to the semifinals, with ten teams finally battling it out for the top prize at the last stage.
One amongst those hundred semi-finalist teams was a student from the Manipal Institute of Technology - Debarun Karmakar.
Into the Spotlight
Debarun was (and still is) in the third year of an undergraduate degree in Computer Science. Growing up in Pune, he spent a chunk of his childhood “in and out of hospitals” dealing with recurring health issues, embedding in him a fascination with the world of healthcare. It’s why, for his case study application, he chose to ‘disrupt’ Narayana Health (NH), India’s largest private hospital network.
NH was founded by legendary cardiac surgeon Dr. Devi Prasad Shetty, and has long been celebrated as the gold standard of low-cost, high-quality healthcare on the Subcontinent. Debarun’s decision to take on NH was emboldened by the fact that, anytime he needed inspiration, he could basically saunter out of his dorm room and stroll ten minutes down the road to the campus of Kasturba Medical College (KMC) and it’s equally vaunted chain of partner hospitals in Manipal.

For three months, Debarun did what any good disruptor is supposed to do - he searched for blindspots and vulnerabilities. He spent time at KMC, walking the wards, talking to doctors and administrators, even peppering the leadership of Manipal Hospitals with questions around their biggest headaches and dream solutions, slowly building a picture of how a major healthcare institution actually works from the inside. He got a privileged audience with Viren Shetty, Narayana Health’s CEO, who’d benevolently made himself available as a resource to all the case study teams that had (rudely) elected to take aim at his institution.
These conversations were illuminating. After passing by the kinds of pointed complaints that sit at the edges of Indian healthcare (lengthy receivables cycles, delays in discharges, limited personal attention from doctors at busy hospitals etc), he finally arrived at the fault line that runs through the entire system.
Case/Build
The big problem - the one that was upstream of so many other problems - was the structural tug-of-war between payer and provider: insurers, patients, doctors and hospitals who weren’t just separate parties, but whose financial survival depended, in ways large and small, on outcomes that were fundamentally at odds with each other.
What does that really mean?
As Debarun found, here’s a mundane example that plays out in hospitals across India every day: A patient comes in with a complaint. Tests are ordered, specialist doctors are consulted, an admission is recommended. Each of these decisions may be entirely legitimate, but each one also happens to generate revenue for the hospital and the doctor. The insurer, on the other side, is looking for any reason to limit the payout (finding the exclusion clause, the pre-existing condition, the technicality that limits the payout etc). So one half of the system is economically oriented to doing more, rather than better, while the other half is looking for ways to pay less. Nobody in this transaction is behaving illegally or even unethically. Hospitals aren’t villains, doctors aren’t charlatans, and insurers aren’t cartoon antagonists. They’re just each defaulting to the incentives imposed by the structural reality they operate within. The trouble is that those incentives don’t always align with yours.
By the way, this isn’t just a mundane example, it’s an entirely ubiquitous dynamic found not only in India but in virtually every for-profit healthcare market in the world. It’s a tension that serious money has been working to resolve for decades. In the US, Kaiser Permanente has operated a fully integrated payer-provider model since the 1940s - and with 13 million members, 55 hospitals, and $115 billion in annual revenue, it remains the most compelling proof that the model really works. It’s why companies like CVS Health, America’s largest pharmacy chain, spent $69 billion acquiring Aetna, one of the country’s biggest insurers, in 2018. Closer to home, Narayana Health itself had arrived at the same conclusion — launching its own standalone insurance product, Narayana One Health, in mid-2024, becoming India’s first hospital-owned insurance brand. The execution has proven harder than expected.
For a potential disruptor looking at this situation from the outside in, the flaw is obvious - and so is the opportunity. If the root problem is that payers and providers are separate entities with misaligned incentives, the solution writes itself: smush them together in the same entity.
What you’d get is one company that insures you, employs your doctors, runs your diagnostics, and maybe even owns your hospital - so that the most profitable thing it can do is also the best possible thing for you i.e. keep you healthy, keep you out of hospital, and never give you a reason to make a claim. Any amount spent on your health and wellness is a cost that pays for itself - a teleconsult today is cheaper than a hospitalisation next year, a preventive screening now is cheaper than a chronic disease later, and a fitness tracker is considerably cheaper than a cardiac surgery. In practice, it could look something like a ‘Spotify for healthcare’ - a single monthly subscription that gives you unlimited access to consultations, check-ups, and diagnostics, underwritten by an entity that makes more money the healthier you stay.
On paper, it is an elegant solution. It’s also a solution that formed the heart of Debarun’s case study submission to The Ken - his theoretical disruptor to Narayana Health - something that looked like a ‘Kaiser Permanente for India’. He didn’t make it past the semifinals, but he left convinced there was something concrete here, something worth building on.
The good news was that he had discovered a genuine opportunity - a real problem in a massive industry (two massive industries), that an entity with no incumbent baggage could conceivably exploit. Unlike the US, no legacy institution had cracked this model at scale in India, and the door was wide open for exactly the kind of new entrant Debarun was imagining. The bad news, as he soon discovered, was that someone else had already walked through it.
Breaking Even
‘Two Italians and an Indian with no medical expertise walk into a hospital…’ is probably a serviceable premise for a joke somewhere in the world. In the case of Even, it has proven a surprisingly excellent premise for a healthcare startup in India.
Even Healthcare was founded in 2020 by the trio of Mayank Banerjee, his friend and former co-founder (at news media startup Compass News) Matilde Giglio, and her childhood best friend and machine learning engineer Alessandro Ialongo.

The apparent disconnect between their backgrounds and their choice of business makes more sense when you consider that the ideological foundation of Even isn’t rooted in healthcare at all - it’s rooted in fairness.
For Mayank, a personal tragedy in his teenage years had made him viscerally aware of how the outcome of a medical emergency in India often hinged more on who you knew and how much money was in your pocket, rather than the quality of care you received and how badly you needed it. Healthcare was an apparent luxury for so many on the Subcontinent, with 5.5 crore (55 million) Indians being thrust into medical bankruptcy every year because of a single hospital bill. So despite spending his formative years in the UK, he moved back to India, to Bangalore, on New Year’s Eve in 2018, determined that India - with its scale, its urgency, and the sheer number of people on the wrong side of fairness, presented a more dire set of problems-worth-solving than anywhere else in the world.
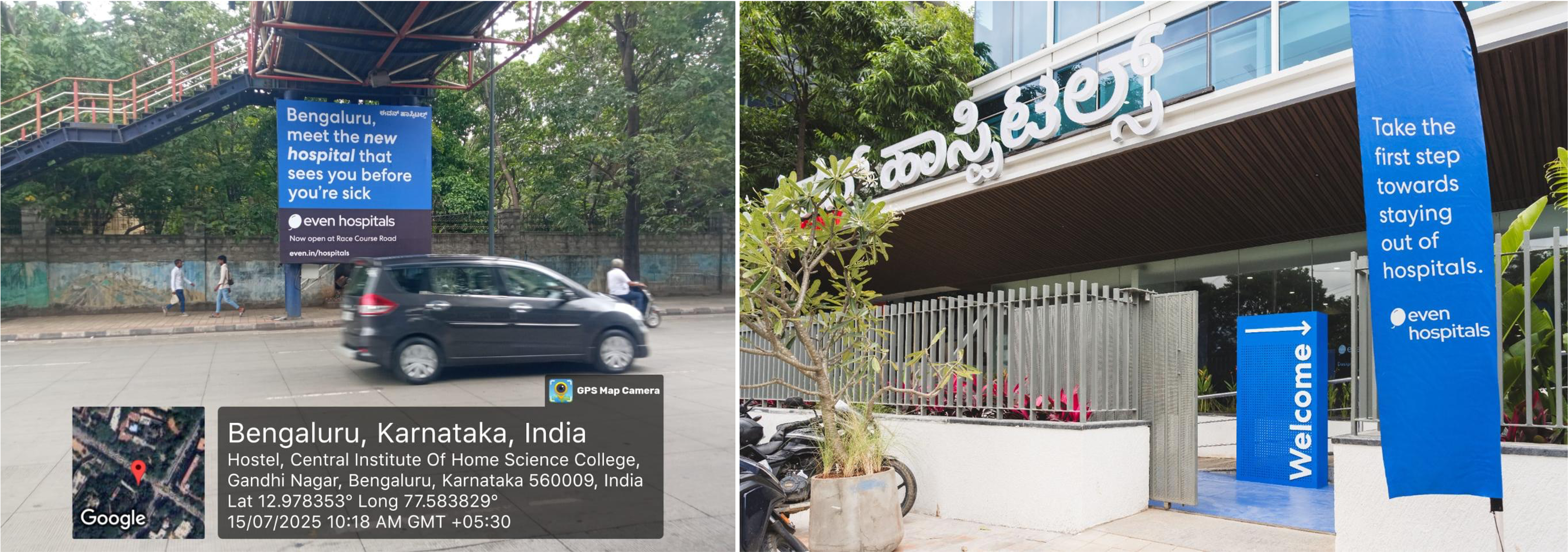
Eventually joined by Matilde and Alessandro in 2020, Even began its operations by offering customers a hospital membership plan - pay a fixed monthly fee, and your hospital bills are covered across their partner network. Today, after five years in the idea maze, their offering has morphed into something closer to a universal healthcare subscription - a single plan that covers unlimited doctor consultations, unlimited diagnostics, and a hospitalisation cover powered by their insurance partners in the background. To fully deliver on their promise and align the focus of every participant in their value chain, Even employs its own team of doctors and specialists across its own network of clinics and diagnostic centres — culminating in mid-2025 with the opening of its first hospital on Race Course Road in central Bangalore, built from scratch in seven months, with several more already in the pipeline.
To us, Even is an Indian startup (and story) that merits close examination, because if all rolls their way, what they hope to have produced over the next 5-10-15 years, is not just a single successful company. What they hope to prove is the viability of a new model for healthcare in India, one that is more equitable, profitable, and replicable than anything that exists right now. Those are the stakes.
But despite all this activity and ambition, Even is in the curious position of being perhaps more well known in San Francisco than it is in India. That’s partly because its work so far has been concentrated within Bangalore, and partly because it sits in the portfolios of several of Silicon Valley’s investing heavyweights. As of the closing of its most recent $20 million round in January 2026 (bringing its total funding to $70 million), Even counts on its cap table Vinod Khosla’s Khosla Ventures, Joe Lonsdale’s 8VC, and Physical Intelligence’s Lachy Groom, among other Indian and American tech luminaries, and carries the distinction of being the only Indian company currently in the portfolio of Peter Thiel’s Founders Fund.
It would be fair to say, though, that it’s not a household name in India yet. Which makes it, for now, a company that’s flown a little bit under the radar of the wider tech ecosystem. It means its disruptive business model has yet to be appreciated outside the healthcare ecosystem, even if you were the kind of person specifically looking for ways to disrupt the Indian healthcare industry…
How We Got Here
“All the ideas I had for new healthcare business models, it felt like Even was already implementing all of them,” says Debarun. “They were somehow reducing costs, improving outcomes, and reducing readmissions, and making it make business sense for themselves and their partners.”
As he dove further into his research on payer-provider business models after bowing out of the case study competition, Debarun finally discovered the work being done by Even and other pioneering Indian healthcare startups, like Varun Dubey’s Superhealth. He turned all of this research, including his primary findings on the problems ailing Indian hospitals and insurers, into a biting 20,000-word Substack post titled ‘The Hospital Rake’. He then put this essay to work, using it as the centrepiece of a cold email to Even’s Mayank Banerjee.
It worked.
Mayank was blown away by the piece, and immediately shared it with his co-founders. “He understood the different pieces of our operation and how they all fit together,” he recalls. “It’s something that usually takes multiple hours and conversations with investors. He knew what we were trying to accomplish in the short term, and correctly surmised what our long term plan was. It was the best thing anyone had ever written about us.”
The Even team invited Debarun to join them as part of the Founder’s Office for the duration of his December break from college. He packed his bags and moved to Bangalore shortly thereafter.
Coincidentally around the same time, we started chatting with Mayank about doing a Tigerfeathers piece on Even in early 2026. During those conversations, Mayank told us about ‘this college kid who’s written this awesome piece on Even that’s worth checking out’. We did. We were impressed.
The writing was sharp, the thinking was clear, the ideas were fresh and opinionated, and the author didn’t have to use any juvenile memes to get his point across.

Outside of any of that stuff, it was just fun to read, and you could tell the author enjoyed creating it too. Around 500 words in, it became clear that 1. there was no way we were writing a better piece on Even or on healthcare in India; 2. this was clearly an exceptional writer writing about a subject he was super passionate about.
You also have to be a little dumb to expect people to read a 20K-word blogpost in 2026, so it came as no surprise to us that he was a longtime Tigerfeathers subscriber (the only thing that worked against him). We reached out to him in December and asked if he would do a v2 of his original essay as a Spotlight piece once his stint with Even ended, presumably informed and sharpened by his time inside the company and his subsequently acquired first-hand knowledge of Indian healthcare, with an expanded scope that included:
Researching the colonial origins of the Indian healthcare system, and explaining why it was never actually designed to cater to the people it currently serves
Unpacking the structural economics of hospitals and insurers, and the perverse incentives that make everyone in the chain behave rationally while the patient pays the price
A rigorous autopsy of why every attempt to fix the value chain has fallen short in the same predictable ways, and how the system often fails the most vulnerable of Indian patients
Why the Even story is different and important - the origin, the model, the near-death experience, and what it means to build a hospital
Why the incumbents can see exactly what Even is doing but can’t just copy it, and what all of this means for the future of healthcare in India
That’s what today’s piece is.
It has taken almost three months, several edits, and an insane amount of work to get here. What Debarun’s produced is a 28,000-word monument to the past, present and future of Indian healthcare - to what is broken, what is promising, and what is at stake.
It is a testament to what happens when someone honours their curiosity by following the thread all the way to the end. It’s the kind of piece that will make you look at the world a little differently, or at least at a tiny part of it. We are all the more grateful for the effort he’s put in given the start of his mid-term exams this past Monday (if any of his teachers are reading this, pls dear sir/madam give this man THE BEST GRADES ONLY - he deserves it).
Anyway, we hope you enjoy reading it as much as we did. This is almost certainly not the last time you hear from Debarun this year. We’ve basically brought him into the Tigerfeathers fold to contribute to what we’re doing on the media and investing front this year (at least until he gets bored or too busy with college work). Watch this space for more from him👀.
With that said, lets get on with it.
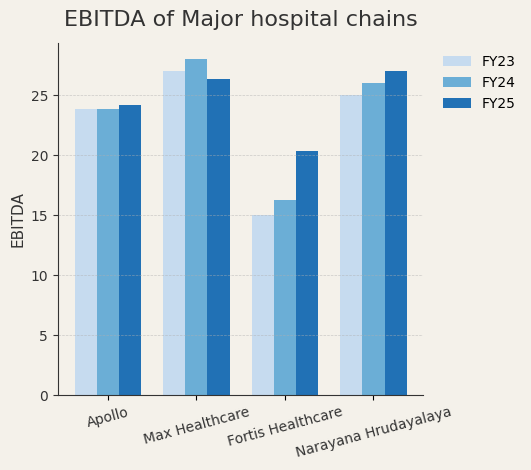
Hey Tigerfeathers readers, Debarun here. Here’s a quick note on methodology before we get started: This piece draws on financial filings from publicly traded hospital chains and insurers (Max, Fortis, Apollo, Star Health), Even Healthcare company interviews and operational data, published research on integrated care models (Kaiser, Optum, Hapvida), IRDAI regulatory data, and WHO/National Health Accounts data on Indian healthcare spending. We’ve toured Even’s hospital, interviewed leadership, and reviewed internal financial models. Some specific numbers are approximated or withheld to protect company confidentiality. Where this creates uncertainty, we’ve noted it explicitly.

[I] What Does the Perfect Business Look Like?
There’s a business model that gets pitched in private equity meetings that sounds, on paper, like the most beautiful thing in the world. The cash flows arrive like clockwork, the customers have zero bargaining power, the physical infrastructure creates a moat, and the total addressable market is…literally everyone.
To top if all off, the return on capital employed is magnificent, and the EBITDA margins are north of 25%.
We are talking about a veritable multi-decade compounding machine. Also known as a hospital.

Let’s diagram a simple, commonplace transaction in the Indian healthcare market. You have two parties: a Creditor and a Debtor.
The itemised bill reads:
Cardiac catheterisation and stent: ₹2,20,000
Two nights in ICU: ₹1,50,000
Diagnostic imaging (ECG, stress test, angiogram): ₹95,000
Medications and pharmacy: ₹45,000
Doctor consultations and fees: ₹34,000
The number on the paper sums up to ₹5,44,000. Roughly $6,000.
It’s a large part of your annual income, which is inconvenient, because you hadn’t planned a major medical event between rent and groceries.
Your mother came in with chest pain. The doctors ran tests. Good tests. Thorough tests. An ECG, a stress test, a full cardiac panel, imaging. The cardiologist expressed “clinical concern,” which is a professional term that often precedes doing a lot more things that involve expensive machines. They did an angiogram, found a blockage, and put in a stent.
Two nights in the ICU, some pills, and a few follow-up appointments later, your mother is stable. The care was excellent. The facility was clean. Everything worked exactly as it should.
Except the bill.
You ask the only question available: “Is all of this necessary?”
The billing administrator looks at you with practiced sympathy. She didn’t make up the price. She’s showing you line items that all have medical codes, approved procedures, standard rates. The doctor followed protocols, ordered appropriate tests, and made clinically sound decisions. The hospital didn’t build expensive cardiac catheterisation labs for fun. These machines cost crores, and once they exist, they need to be used to justify their existence and pay back the debt that financed them.
Everyone is more or less doing their job.

This is not a story about bad people and evil math. This is a story about good people and unfortunate math.
Hospitals cost a lot to build and run, and once they exist, the sensible financial move is to use them as much as possible. When the hospital runs more tests, does more procedures, keeps you for extra observation days, i.e. when more billable things happen to you, more capital gets repaid. The MRI machine’s loan gets paid down a little faster. The catheterisation lab justifies its existence. The building moves closer to profitability. It’s just how the system is wired.
None of this is visible to you, standing in the corridor outside your mother’s room, holding a piece of paper with ₹5,44,000 printed at the bottom. You’re not thinking about debt service schedules or utilisation rates. You’re thinking about how a number this large appeared at the end of what felt like completely normal medical care, and whether any of it was actually necessary, and whether “necessary” is even a question you’re allowed to ask at this point.
But wait…what’s that in your back pocket? It’s…Insurance. You have insurance. Thank god. You’ve been paying ₹18,000 annually for the last three years for exactly this situation.
The insurance company reviews the file. Several procedures are being questioned.
“Medical necessity not established for pre-procedure imaging.”
“Observation period exceeds standard protocol for this intervention.”
“Pharmacy charges include non-formulary medications.”
“Claim partially denied. Approved amount: ₹2,69,000.”
Your responsibility: ₹2,75,000.
You call the insurance company. The representative is polite but firm. The policy has terms, you see. The hospital billed above standard rates. Some procedures weren’t pre-authorised. But don’t worry, there’s an appeals process if you disagree.
You call the hospital. They explain they can’t negotiate the bill downward, policy determines rates, and you received the care. If you had concerns about costs, you should have discussed it before the procedures.
Neither party is lying. Both are following their rules. The outcome is that you’re out ₹2,75,000 for your mother’s heart problem, and you’re not even sure which parts were “necessary” and which parts were “hospital needs to justify expensive equipment.”

Now comes the part nobody tells you about in the glossy hospital brochures.
₹2,75,000 is not a number that exists in your bank account. Your household brings in ₹8 lakhs a year. You have maybe ₹40,000 in savings. The hospital knows this, has always known this, because the ‘Estimate Desk’ (more on this later) clocked you the moment you walked in without a car, reading the specific kind of anxiety that signals limited liquidity.
Your mother is medically cleared to leave. But the discharge paperwork sits unsigned on the administrator’s desk. The insurance has paid its portion. The remaining ₹2,75,000 must be settled before she goes anywhere. This is not a negotiation. It is a countdown. Seventy-two hours.
What happens next is a forced liquidation event that plays out in millions of Indian households every year:
Your father makes calls to family members. An uncle in Mysore has a Provident Fund he can borrow against, but the paperwork will take four days and there’s a 10% penalty. Your brother-in-law has a mutual fund investment, ₹1.2 lakhs, but redeeming it now means a 15% short-term capital gains hit. Your mother’s brother offers to sell some agricultural land, the family’s only appreciating asset, but in a fire-sale it will fetch maybe 60% of its actual value.
You pool these emergency liquidity sources like you’re assembling a ransom payment. Because functionally, that’s exactly what this is. The hospital has something you need - your mother’s discharge and dignity and the price is non-negotiable.
Three days later, you return to the billing office with a bag containing:
₹80,000 in cash withdrawn from your father’s PF (with penalties)
₹1,00,000 from your brother-in-law’s liquidated mutual fund
₹95,000 from the distress sale of farmland that’s been in your family for two generations
The hospital administrator counts it, generates a receipt, and hands you the discharge summary. Your mother can leave now.
This transaction, from the hospital’s perspective, is a masterclass in operational excellence. Zero receivables. No payment plans. No defaults. Cash on the barrel, collected at the point of maximum leverage. The hospital’s balance sheet records this as “revenue,” and the family’s balance sheet records this as “catastrophic health expenditure,” but these are just two ways of describing the same transfer of wealth.
The medical emergency is over. The financial emergency has just begun. The mutual fund that was meant to fund your brother’s wedding is gone. The farmland that was supposed to be your parents’ retirement security is gone. The Provident Fund that was your father’s hedge against unemployment is depleted.
You did what you had to do. And so did fifty-five million other Indian families this year.
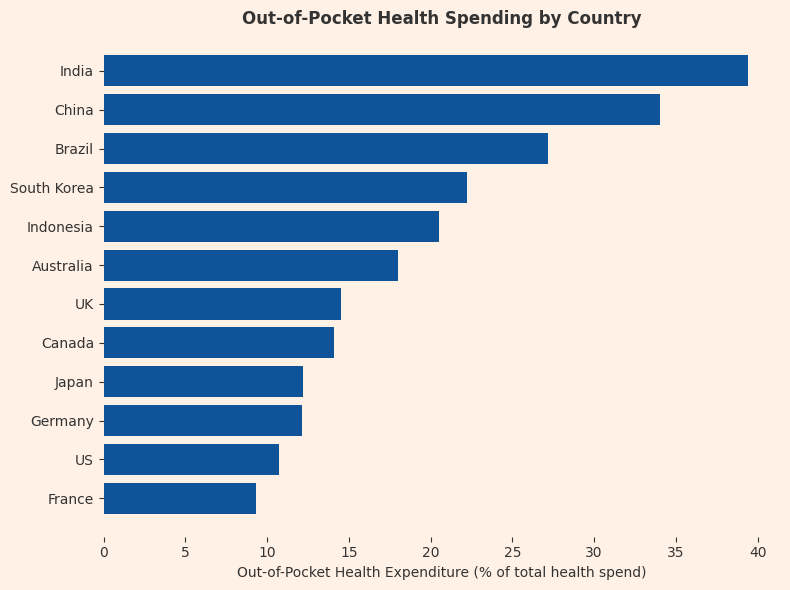
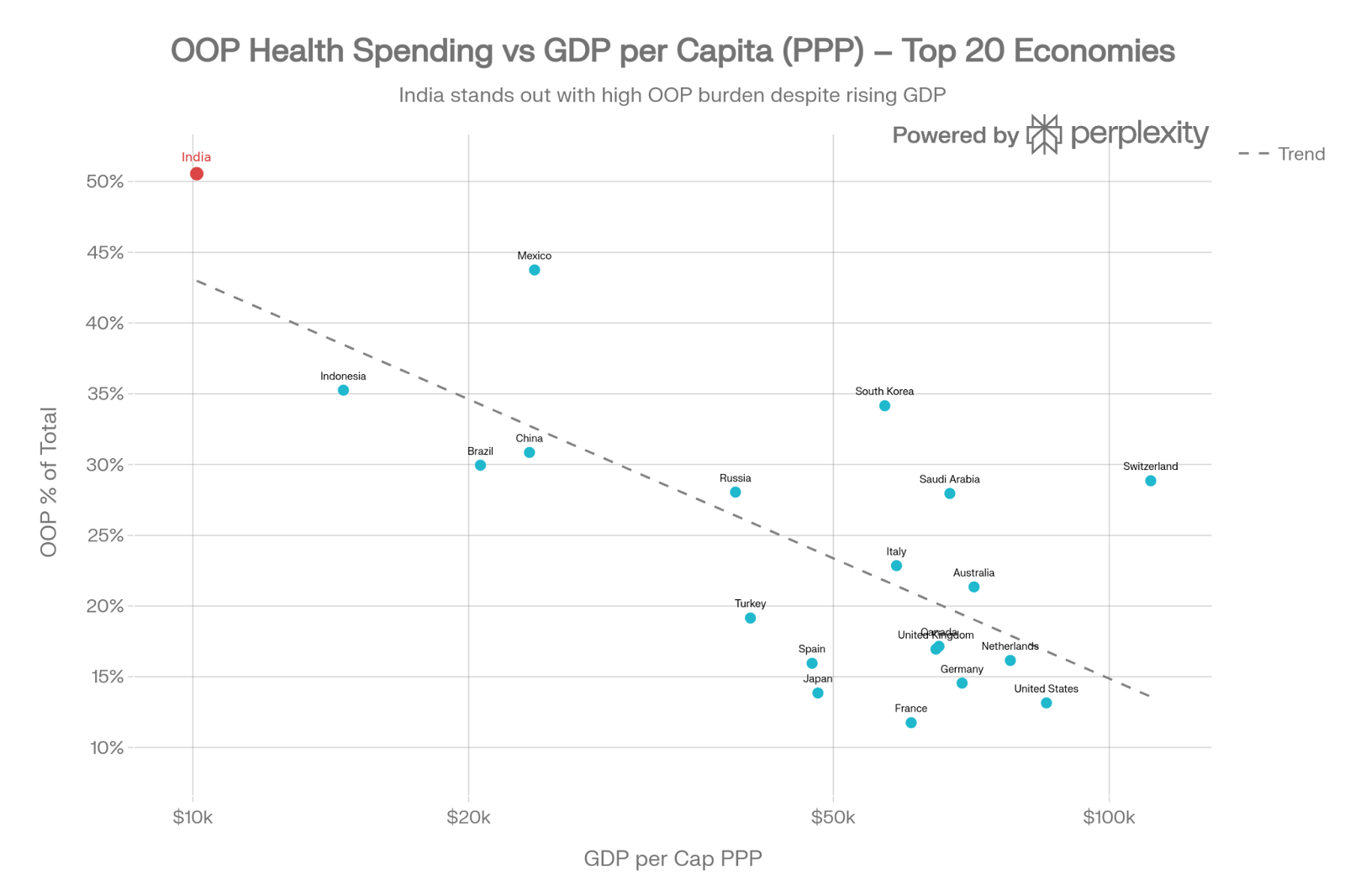
Now scale this single transaction from above across a country of 1.4 billion people and the macro picture starts to look a bit extreme.
India funds roughly 39.4% of its healthcare the old-fashioned way, by reaching directly into wallets at the worst possible moment. Every year, more than 55 million Indians face medical bankruptcy. That’s the entire population of Canada being pushed below the poverty line annually because someone got sick.
And here’s the part that should make you close your laptop and stare into the void: all of this means private hospitals are excellent businesses.
The distinction matters. Public hospitals in India operate under an entirely different logic - chronically underfunded relative to need, they nonetheless serve the majority of India’s population and remain the primary option for hundreds of millions who have no private alternative.
The private hospital sector, which now accounts for roughly 70% of all healthcare delivery in India, operates under an entirely different logic.
Demand is steady and rising. Supply is structurally constrained. Prices are opaque. The customer rarely chooses based on cost. Payment is increasingly routed through insurers and governments, which dulls price sensitivity further, but when it fails, the collection mechanism we just witnessed kicks in with brutal, mechanical precision. In almost any other industry, this would be described as pricing power.
And hospitals sit at the centre of that dynamic. They control the physical assets (the beds, the machines, the expertise). They control the moment of maximum leverage (the emergency, the discharge, the “estimate desk”). They control the information (what’s necessary, what’s standard, what’s negotiable). They are simultaneously the service provider and the debt collector, the caregiver and the creditor.
The system isn’t failing. It’s doing exactly what it was designed to do - optimise throughput, billing, and utilisation. Health just isn’t one of the variables it’s rewarded for improving.
You can’t fix this by asking hospitals to act against their own economics. You have to change who holds the risk, who controls the assets, and when money is made. You have to redesign the system so that the most profitable thing to do is also the healthiest thing for the patient.
But to understand why that’s so difficult, you need to understand how we got here.
[II] The Original Sin
The Accidental Enterprise
If you want to understand why Indian healthcare works the way it does, you have to realise that it isn’t really one system. It’s a series of historical accidents that someone eventually tried to turn into a business.
To understand this dysfunction, we have to go back to the era when healthcare was an HR function of the British Raj. The colonial government did not build healthcare in India to “help people”, rather it was designed to keep the colonial administration from dying. If you are running an empire, you need a repair shop for your administrators and your military. So, you build hospitals in the places where your employees happen to live - and in the mid-nineteenth century, that meant the three great presidencies: Bombay, Calcutta, and Madras.
Let’s take Calcutta. The Medical College of Bengal, established in 1835, was the the first institution in Asia to teach modern Western medicine. But although it was built in the empire’s most important city it was not built to serve the city’s millions. Instead, its purpose was to ensure a British officer didn’t die of infectious disease before his pension vested.
Over on the west coast, Bombay got the Grant Medical College. Founded in 1845, it was a grand institution with marble floors, European-trained surgeons, and imported equipment. The standard of care matched what you would find in London. But the logic underpinning it was the same: keep the rulers functional, ignore everyone else.

After independence, India inherited this template. It was not dissimilar to inheriting a corporate campus designed by a company that went bankrupt in 1947: the plumbing is weird, the buildings are in the wrong places, and it was never actually intended for the people who live there now. The hospitals existed, but they were positioned for the needs of a departed empire, not a newly independent nation of 300 million people spread largely across disconnected villages and towns.
The Promise Of The Committee
In 1946, the Bhore Committee, led by Sir Joseph Bhore and tasked with planning India’s health infrastructure from first principles, spent two years studying the country’s health needs and produced a vision so comprehensive it filled four volumes.
The report was extraordinary in its ambition and clarity. It envisioned a complete transformation: a national program of health services that would reach every village, integrate preventive and curative care, and train a new generation of “social physicians” who understood that health went beyond just treating disease and extended to sanitation, nutrition, and prevention.
The committee’s most striking passage captured both the scale of the problem and the urgency of the solution:
“If it was possible to evaluate the loss, which this country annually suffers through the avoidable waste of valuable human material and the lowering of human efficiency through malnutrition and preventable morbidity, we feel that the result would be so startling that the whole country would be aroused and would not rest until a radical change had been brought about.”
They weren’t wrong about the loss. What they underestimated was how difficult it would be to arouse the country, or more precisely, to arouse the country’s budget allocation.

The Bhore Committee proposed a two-stage rollout. Over the short term, one Primary Health Centre for every 40,000 people, staffed by two doctors, one nurse, four public health nurses, four midwives, two sanitary inspectors, one pharmacist, and supporting staff, was recommended for immediate implementation. These PHCs would handle basic care and refer complex cases upward.
The eventual plan was more ambitious: a comprehensive three-tier system with a 75-bed primary unit for every 10,000-20,000 people, feeding into 650-bed secondary hospitals at the district level, which would connect to 2,500-bed tertiary hospitals for the most complex cases. The entire country would be covered by an integrated grid of healthcare facilities, each level supporting the one below it.

But buried in those four volumes, easy to miss between the staffing ratios and bed counts, was a single line that cut to the heart of the matter: “Integration of preventive and curative services at all administrative levels.”
Read that again.
In 1946, a committee of bureaucrats and physicians looked at India’s healthcare problem and concluded that the only real solution was to stop treating prevention and treatment as separate activities, that the doctor who kept you healthy and the doctor who fixed you when you weren’t should be part of the same system, with aligned incentives and shared information.
They saw it clearly. They wrote it down. They put it in an official government report.
The report was a masterpiece of central planning. On paper, it was exactly what India needed: a rational, hierarchical system that could deliver care at scale while managing costs through appropriate triage and referral.
The government drew up maps and began implementation. By 1952, India established its first Primary Health Centre. By 1961, there were 2,800 PHCs dotting the country. By 1981, that number had grown to 5,300. On a map, it looked like the Bhore Committee’s vision coming to life, neat dots representing clinics scattered across the country, a grid of care covering the subcontinent.
The middle tier - district hospitals meant to bridge the gap between primary care and specialist treatment - got built too, after a fashion. Most major districts eventually had a government hospital. The buildings existed. The beds existed. But chronic underfunding meant they operated as overwhelmed referral dumps rather than the coordinated secondary care facilities Bhore had envisioned. A district hospital in rural Uttar Pradesh in 1975 was less a functioning healthcare institution than a place where PHC failures went to be confirmed.
The top of the pyramid told a different story. The All-India Institute of Medical Sciences, established in New Delhi in 1956, was genuinely world-class - a tertiary care institution that could hold its own against the best hospitals anywhere. AIIMS became a symbol of what Indian healthcare could be when properly funded and properly run. The government went on to build six more AIIMS campuses over the following decades (until 2014, after which the government built or sanctioned 20 more). They remained islands of excellence - exactly the colonial paradigm the Bhore Committee had set out to dismantle, now reproduced in independent India’s own image.

So why didn’t we scale to create an archipelago of islands? One constraint stood in the way: the budget.
The 1% Solution
Post-independence, the new government made healthcare a cornerstone of its socialist promise. The commitment wasn’t accidental - Article 47 of the Indian Constitution, adopted in 1950, explicitly directed the state to raise the level of nutrition and standard of living of its people and improve public health. It was a founding obligation, written into the document that defined what independent India was supposed to be.
Here’s the problem with promising healthcare as a constitutional directive: directives require funding, and funding requires political will that survives contact with competing priorities. India’s government health spending has hovered around 1% of GDP for decades. For context, that is about what you’d spend if your plan was “hope nobody gets sick.” Middle-income nations usually spend 4-6%. Even other developing countries in the 1970s and 80s were spending 2-3%.
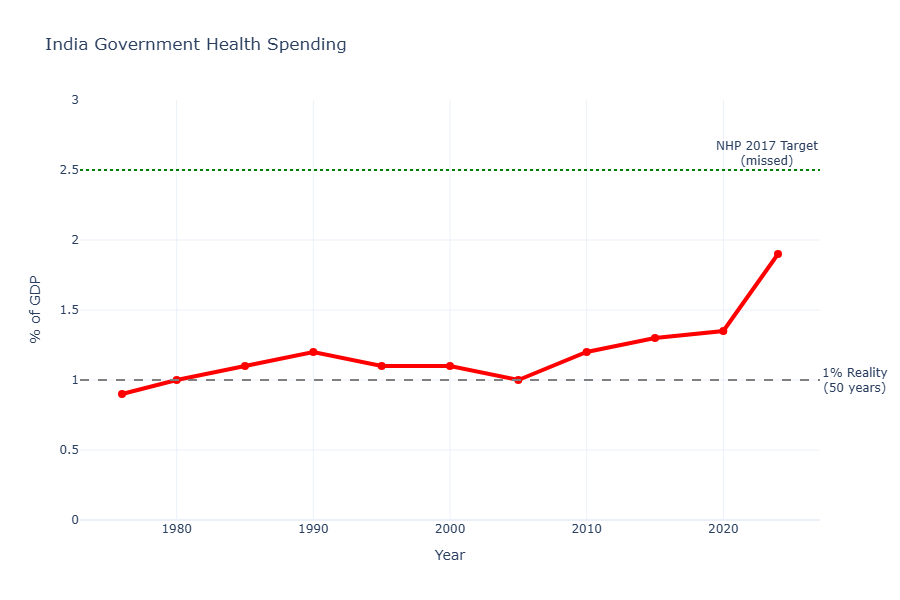
If you promise “Right to Health” but only fund 20% of what’s actually needed, you haven’t created a right. You’ve created a very expensive system to let people down.
On January 26, 1951, India’s second Republic Day, Rajkumari Amrit Kaur, the nation’s first Health Minister, published an essay describing what was already becoming clear.

Just three years after independence, she wrote:
“It is a real tragedy for India that very little attention has been paid to the nation’s health in the past... Independent India has had, therefore, to face a tremendous problem... We have got practical projects which we would like to undertake but we are handicapped by financial stringency.”
She catalogued what states were attempting: West Bengal launching hospital schemes on Bhore Committee lines, Uttar Pradesh opening rural dispensaries, Bihar experimenting with preventive health units. She described the tuberculosis crisis - 2 million sufferers, only 6,000 beds in 1947, doubled to 12,000 by 1951. Still serving less than 1% of those who needed them.
She acknowledged that “only a very small fraction of the revenues of the Government have in the past been devoted to Health.”
Then she ended with optimism: “The Ministry is confident that with the co-operation of the public and the medical profession, India will achieve a standard of health which will be the envy of other nations.”
She was describing, in real-time, the moment when the Bhore Committee’s comprehensive vision collided with “financial stringency.” The gap between “projects which we would like to undertake” and actual implementation would only widen over the next three decades.
The PHCs were built, or at least, buildings with “PHC” painted on them appeared in villages. But the buildings were shells. The doctors were missing, either never hired or hired and immediately transferred to cities where life was easier and corruption more lucrative. The medicine was perpetually out of stock because the procurement system was designed for bureaucratic compliance, not actual supply chain management. The equipment was broken, and stayed broken, because there was no maintenance budget and no one wanted to take responsibility for fixing anything.
?")
In the 1980s government studies found that 30% of PHC positions were vacant. In some states, the number was closer to 50%. The doctors who did show up often ran private practices on the side, treating government service as a part-time obligation. The “compulsory rural posting” required of new medical graduates became an elaborate game of connections and bribes to secure transfers to urban areas.
By the 1970s, a typical PHC looked like this: a concrete building, often well-constructed, sitting empty or staffed by a single underpaid nurse who showed up twice a week. The “doctor” listed on the books lived in the district capital and hadn’t visited in months. The medicine cabinet contained expired paracetamol and some dusty bandages. If you showed up with a serious illness, you were told to go to the district hospital 40 kilometres away, which had its own problems - no beds, no specialists, equipment that hadn’t worked since installation.
The rural poor, the people this system was ostensibly built for, quickly learned that the PHC was a place you visited if you wanted your time wasted. For anything serious, you borrowed money and went to a private doctor or traveled to a city hospital.
The gap between promise and reality became so vast it was almost comic. Government reports would dutifully count the number of PHCs established, the number of beds added, the quantity of medicine procured. None of these numbers bore any relationship to whether an actual sick person could actually receive actual care.
The system excelled at producing statistics. It failed at producing health.
The Great Exodus
By the 1980s, India’s public health system had become something paradoxical: it wasn’t a healthcare delivery mechanism as much as it was a “credentialing infrastructure” for doctors.
Medical colleges, many of them government-run, produced tens of thousands of doctors annually. These doctors were required to do a rural posting, a year or two in a PHC to “serve the nation.” But when these doctors arrived at their assigned PHCs, they found buildings with no medicines, no equipment, no support staff, and no functioning systems. They were expected to treat patients with nothing.
Some tried. Most realised quickly that the public system was designed to fail.
The moment their mandatory service was complete, they left. They went to cities and started private practices. They joined corporate hospitals. They went abroad. The public system became, in effect, a taxpayer-subsidised training program for private healthcare. The government paid to educate the doctors, then watched them leave because the system it built was impossible to work in.

The doctors who stayed in the public system were either exceptionally dedicated or had no other options. The result was a bifurcation: competent doctors left for private practice where they could actually practice medicine and earn a living, while the public system retained a hollowed-out workforce operating in hollowed-out buildings.
For patients, the message was clear: if you wanted competent healthcare, you paid for it privately. The public system was what you endured when you had no other choice.
Who Steps in When the Government Steps Back?
Then came 1991 and liberalisation.
The economy opened up. GDP growth accelerated, 6-8% annually through much of the 1990s and 2000s. The middle class expanded dramatically. By 2000, roughly 50 million households had crossed into middle-class income levels. By 2010, that number had doubled. Disposable incomes were rising. People had money to spend on healthcare.
And the government was still spending 1% of GDP on empty PHCs.
The state, which had promised to provide healthcare, effectively vacated the field. Not through explicit policy, but through sustained neglect. The public system continued to exist in theory - the PHCs and district hospitals remained on maps, budgets were allocated (and often unspent or siphoned off through corruption), but in practice, the government had stopped trying to deliver healthcare at scale.
This created a vacuum.
And if there is one thing capital hates, it is a vacuum where people are willing to pay money to not die.
Private capital rushed in.
Between 1990 and 2010, private capital poured into Indian healthcare with the kind of enthusiasm usually reserved for gold rushes. Private hospital beds grew rapidly during this liberalisation era. In the last five years alone, $15 billion flowed into the sector. If you plotted healthcare investment on a graph, it would look like a hockey stick.

But here’s what’s strange: despite all that capital, despite all those new beds, supply remains structurally constrained. India still has only 1.3 hospital beds per 1,000 people, less than half of what the WHO recommends and a fifth of what China has built.
So, where did the money go?
The answer reveals something fundamental about how capital behaves when it’s rational.
If you give private equity a choice between:
Option A: Building a network of primary care clinics in tier-2 cities that prevent diabetes through patient education and routine monitoring, or
Option B: Building a 500-bed specialty hospital in Bangalore that does robotic cardiac surgery and orthopaedic procedures for patients with high-limit insurance...
...they will choose Option B every single time.
And for excellent reasons.
Option A generates thin margins (8-12%), requires constant patient acquisition, depends on high volume to break even, and pays back capital over 7-10 years.
Option B generates 25% EBITDA margins, has predictable utilisation from a wealthy patient base, attracts doctors who want to work with cutting-edge equipment, and pays back capital in 4-5 years.
The math is brutally clear. Between 2015 and 2020, India added roughly 50,000 private hospital beds. The vast majority went into tertiary care facilities in major metros - Delhi, Mumbai, Bangalore, Hyderabad, Pune. You can now get robotic prostatectomy, complex cardiac ablation, or advanced oncological treatment performed by surgeons trained at Johns Hopkins, Mayo Clinic, or leading European institutions.
But if you live in Indore or Bhubaneswar and need basic diabetes management, maternal health monitoring, or routine preventive care? Your options remain limited. The neighbourhood clinic with a qualified GP doing systematic chronic disease management barely exists outside the top-tier cities.
The infrastructure that was built reflects capital allocation logic, not population health needs. We first built world-class repair shops for the British gentry in colonial India. Then we built patchwork primary health centres for the many. And now we have a healthcare system optimised for the fortunate urban few in the post-liberalisation era.
The care infrastructure for everyone else remains fragmented across thousands of independent private clinics with wildly varying quality, no systematic protocols, and no coordination.
This wasn’t malice. It was capital doing exactly what capital is supposed to do: flowing to the highest risk-adjusted returns. The tragedy is that the highest-return projects don’t align with what a billion people actually need.
[III] When Beds Do The Eating 🍽️
There is a theory in technology investing that says value inevitably migrates to the “aggregator.” Ben Thompson of Stratechery, who has written more clearly about platform economics than almost anyone, describes how the internet fundamentally changed competition:
“No longer do distributors compete based upon exclusive supplier relationships, with consumers/users an afterthought. Instead, suppliers can be commoditized leaving consumers/users as a first order priority... The most important factor determining success is the user experience: the best distributors/aggregators/market-makers win by providing the best experience, which earns them the most consumers/users, which attracts the most suppliers, which enhances the user experience in a virtuous cycle.”
In this view, software eats the world by controlling the users and commoditising the underlying assets. If you control the travellers, you control the hotels. If you control the searchers, you control the websites.
It turns out that when there are 1.4 billion people and very few hospital beds, the beds do the eating.

Indian healthcare has spent the last five years as a brutal, multi-billion-dollar lesson in supply-side economics. You cannot “aggregate” demand for an ICU bed when there are only 1.3 beds for every 1,000 people. You cannot commoditise scarcity. In a market where people are desperate to not die, the person with the physical room and the oxygen tank is the one with the pricing power.
The public markets have priced this reality with a level of enthusiasm usually reserved for companies that sell pixels and have zero marginal costs. India’s top hospital chains trade at 30-50x EBITDA.
I mean, it’s a hospital. It is a building full of very expensive machines and people in scrubs who require salaries. It has all the marginal costs. But if you have the only quality bed in town, the market treats you like a SaaS monopoly.
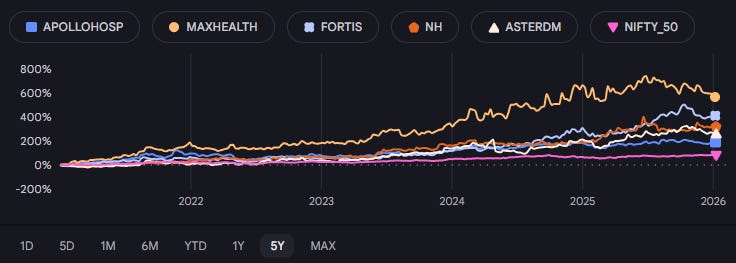
Consider the performance of India’s top five hospital chains - Apollo, Max, Fortis, Narayana, and Aster DM. Over the last five years, this cohort has delivered a 36% CAGR, returning 2.5x the broader Nifty 50 index (~15% CAGR).
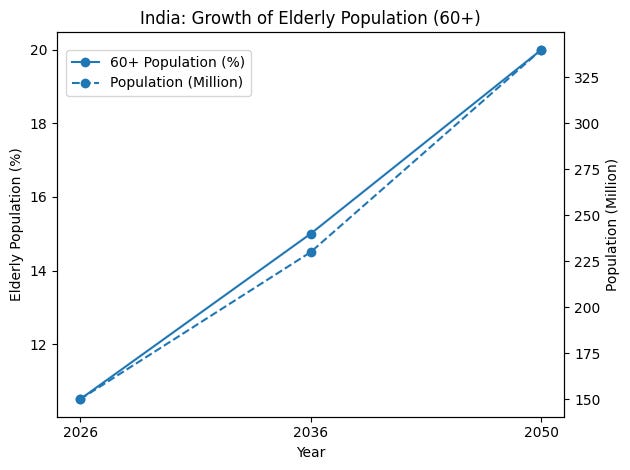
This supply rigidity is currently colliding with a massive demand shock. India is famously young. It has a “dEmOGraPhiC DivIDeNd”. It is a country full of twenty-somethings currently powering the global economy, which is a wonderful thing for GDP. But from a healthcare perspective, a demographic dividend is really just a demographic loan that eventually comes due.
India is aging rapidly in the background. While the world looks at the youth, the 60+ cohort, the people who actually consume the bulk of healthcare resources, is quietly on track to hit 195 million by 2030.
At the same time, the disease profile is shifting in a way that makes the math very attractive for whoever owns the beds. Acute care, ie. getting hit by a bus or catching a one-off infection, is a “bug” in the system. It is episodic and unpredictable. Chronic care for conditions like diabetes or hypertension is a “feature.” It is highly predictable recurring revenue.
If you have 90 million diabetics and 300 million hypertensives, you aren’t running a repair shop for accidents anymore. What you are is something akin to a medical subscription service for an aging population. And in a market with no supply, that is a very good service to be in.
So, Surely There Was A Hospital Boom?
Now, in a normal market, if you saw a business trading at 50x EBITDA, you would expect a massive construction boom. You would see cranes everywhere building new hospitals.

That is not what is happening. Instead, the industry is consolidating. The incumbents are using their capital for M&A, buying up regional players to acquire immediate EBITDA because building a new hospital from scratch involves “regulatory friction” and “gestation risk,” which are professional terms for “it’s a giant headache and takes forever.” Therefore, the preferred playbook remains financial aggregation as opposed to capacity creation.
The approval process requires navigating land acquisition, environmental clearances, fire safety certifications, medical council registrations, and a byzantine web of permissions from multiple government departments that may or may not be incentivised to move quickly. Then you spend 18-24 months on construction, another 6-12 months on equipment installation and staff hiring, and 12-18 months ramping to sustainable occupancy levels.
That’s 3-4 years before you see positive cash flow, during which your capital is tied up earning nothing while accruing interest.
Or you could acquire an existing hospital that’s operating at 60% occupancy, optimise it to 75%, and add ₹50 crores to EBITDA within 12 months without pouring a single bag of cement.
The preferred playbook became financial aggregation rather than capacity creation. Buy existing beds, not build new ones. Roll up regional chains. Extract operational improvements. Show EBITDA growth to justify the 40x multiple.
The result: massive capital deployment, extraordinary valuations, and supply that remains stubbornly constrained.
[IV]The Insurance Inflection
While private capital was building tertiary hospitals and consolidating through M&A, something else was quietly shifting in the background: how Indians thought about paying for healthcare.
For decades after independence, health insurance barely existed. Families were the insurance system. When someone got sick, relatives pooled money. The middle class saved aggressively precisely because there was no other backstop. If a medical emergency hit, you liquidated assets, borrowed from extended family, sold ancestral land if necessary, and hoped the crisis didn’t wipe out three generations of accumulated wealth.
For most people, this was the only option. Until it wasn’t.
Everything Ends Up Being Insurance
Across every economy that has industrialised over the past century, healthcare follows an identical trajectory: all healthcare spend eventually ends up becoming insurance spend.
A plummeting line showing that as countries get richer, “reaching into your wallet at the morgue” is replaced by “paying a premium to an actuary.”
This is the “Everything Ends Up Being Insurance” hypothesis.
Insurance adoption follows the S-Curve, and it describes the exact moment when a society stops asking their relatives for money and starts buying insurance.
Below $5,000 GDP per capita, insurance is a luxury. You spend your money on things like “food” and “not having the roof leak.” If a medical emergency happens, you self-insure through a combination of your savings account and the generosity of your cousins. Above $35,000, insurance is just part of the background noise of being an adult.
The interesting part is the middle. There is a narrow band, roughly between $5,000 and $7,000 per capita, where adoption really takes off. It’s the inflection point where a population decides that paying a monthly premium is a better deal than having a heart attack wipe out a generation of family wealth.
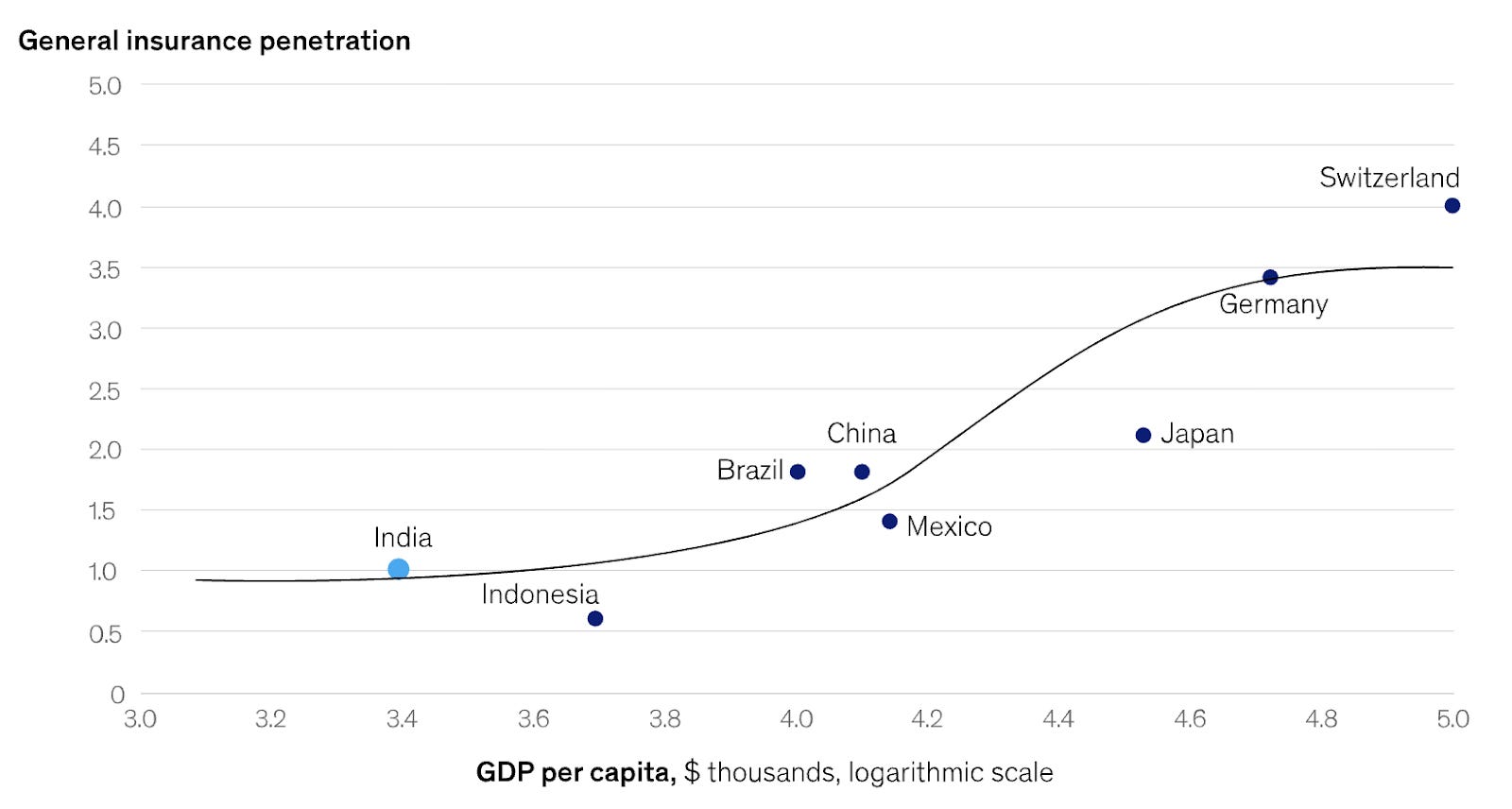
As per the latest figures from the IMF, India sits at approximately $3,000 per capita today, closer to $13,000 when adjusted for purchasing power. Right at the bottom of that steep part of the curve where things accelerate.
If you look at the numbers, the explosion has already started. Health insurance premiums grew from $6.3B in 2019 to $15B in 2024, a 16.8% CAGR over the last five years.

Now before diving into insurance economics, it’s worth noting that the formula for health insurance companies to make money is fairly simple.
Profit = Premiums - (Premiums * Medical Loss Ratio) - (Premium * Admin Ratio)
And just so we’re all on the same page, we’ll do a quick primer on Insurance Economics for a few paragraphs before moving ahead -
In the insurance business, there is a number called the Medical Loss Ratio (MLR), or, if you are being slightly more neutral, the claims ratio. It is a delightfully cynical name. It represents the percentage of premiums that the insurance company actually has to spend on, you know, medical care.
In any other industry, providing the service you sold is called “the product,” but in insurance, it is a “loss.” If you buy a policy and then have the audacity to actually get sick, you are a liability on a spreadsheet.
Then there is the Admin Ratio. This is the cost of everything else: the rent for the glass office tower, the marketing budget for the billboards, and the salaries of the people whose job it is to figure out if your claim can be legally ignored.
If you add these two together, you get the Combined Ratio.
If the ratio is 95%, the insurance company keeps five cents of every dollar. This is a good day at the office.
If the ratio is 105%, the company is literally losing five cents on every dollar of insurance it sells.
On paper, a company with a 105% combined ratio looks like a very expensive, very poorly managed charity. And yet, some of the largest insurers in the world have run these numbers for decades without going bankrupt. They do this by realising that they aren’t actually in the insurance business; they are in the Float Business.

Float is the Warren Buffett special. It is the money sitting in the insurer’s bank account between the time you pay your premium and the time they actually have to pay for your surgery. If an insurer collects ₹100 from you today and expects to pay out ₹105 in five years, they have effectively just taken an interest-free loan from you. Actually, it’s even better than interest-free; if they invest that ₹100 and earn a 7% yield, they make ₹7 in investment income working off your dime.
The math looks like this:
Underwriting Profit/Loss: -₹5
Investment Income: +₹7
Net Profit: +₹2
At that point, you aren’t really an insurance company anymore; you are a hedge fund that uses future claims obligations as a source of interest-free leverage. Warren Buffett calls this a “negative cost of capital,” and it is the best kind of leverage in the world because, unlike a bank loan, you don’t have to pay it back until someone gets sick.
This strategy works beautifully in life insurance or reinsurance, where you can sit on the money for decades (“long-tail” liabilities). It fails spectacularly in health insurance, where the “tail” is short. People get sick fast. You don’t have twenty years to invest a premium meant for a medical event. You have maybe two months.
In India, the “Float Game” is less of a strategy and more of a distant dream, mostly because the bucket is currently empty: retail health insurance penetration stands at just 0.11% of GDP, and total health insurance at a mere 0.3% of GDP.
You can’t run a multi-billion-dollar hedge fund on interest-free leverage if nobody is giving you the leverage in the first place. As we noted, only about 40% of Indians have a personal health insurance policy. When 60% of your population lacks any coverage whatsoever, your “float” is a series of small puddles that evaporate before you can find a broker.
Back to (the Insurance) Business
Because India is sitting right at the bottom of that vertical S-curve, where nominal GDP is $3,000 and 48% of healthcare is still paid for by people reaching into their pockets at the pharmacy, the industry hasn’t reached the level of “financialisation” where you can ignore the underwriting. In a mature market, you can afford to be a slightly incompetent insurer if you are a brilliant asset manager. In India, you have to be a brilliant insurer because the tail is too short and the pool is too small.
The result is that Indian health insurers are stuck in the most difficult version of the game. They don’t have the “long-tail” luxury of life insurance to build a Buffett-style empire, and they don’t have the mass-market penetration to make up for thin margins with sheer volume. They are trapped in a world where they have to make money the hard way: by actually making sure their “Medical Loss” doesn’t swallow the whole rupee.
And since they don’t control the hospital, and they don’t control the doctor, and the “Float” isn’t there to save them, they do the only thing a rational, trapped financial entity can do. They build the trapdoors. They write the fine print. They hire people to say “no.”
They realise that since they can’t be a hedge fund, they have to be a fortress. They protect their 2% EBITDA margin by making sure you never get to see it. It is a perfectly logical response to a structurally impossible position.
In fact, if you look closely at the entire ecosystem, you’ll find that everyone is behaving with the same level of cold, mathematical logic. The system isn’t failing due to bad actors, but because rational participants have done the math and concluded that the current equilibrium is the only way to remain solvent. To fix it, you have to understand that the ensuing madness is actually a form of sanity.
[V] Why Is Everyone Acting Rationally?
The madness starts with a very simple instrument called Fee-for-Service (FFS). It is exactly what it sounds like: you show up, the doctor does a thing to you, and you (or your insurer) pay for that thing. If the doctor does two things, you pay for two things. If the doctor does ten things, like ordering an MRI for a tension headache, you pay for ten things.
In any other industry, this is just how a store works. If you go to a hardware store and buy ten lightbulbs, you pay for ten lightbulbs. The problem is that in healthcare, you don’t actually know if you need ten lightbulbs. You are relying on the guy who sells lightbulbs to tell you how dark it is.
The incentive here is not complicated: if you get paid per “thing,” you have a very strong financial reason to find more “things” to do. This would be fine if more things were correlated with you not dying, but in medicine, the correlation between “total billing” and “clinical health” is essentially a random walk.
This creates a brutal principal-agent problem. You, the patient, are the principal. You want to get better. The doctor is your agent. The doctor is supposed to act in your best interest. But the doctor’s paycheck comes from doing procedures, not from keeping you healthy, so their incentives don’t always align with yours.
Most doctors in India’s private hospital system aren’t actually salaried. They operate under something called a “Minimum Guarantee “(MG), a contract structure where the doctor receives a fixed payment only if they generate a predetermined revenue target for the hospital. If they don’t hit the target, they earn less. If they exceed it, they keep a percentage of the overage.
This is perversely expressed in metrics like “OP/IP conversion ratio”, the rate at which a doctor converts outpatient consultations into inpatient admissions. The doctor is literally judged on how many patients they can convince to get admitted.
Similarly, an orthopedic surgeon, for instance, might receive 30-40% of the revenue from every surgery they perform. Let’s model the choice architecture. A patient presents with knee pain.
Option A: Prescribe physical therapy. Revenue: ₹20,000. Surgeon’s Commission: ₹0.
Option B: Recommend a knee replacement. Revenue: ₹5 lakh. Surgeon’s Commission: ₹1.5-2 lakh.
This is a perfectly designed principal-agent structure. The patient (the principal) wants the best medical advice and medical outcome at the lowest possible cost. The agent (the doctor) wants a good medical outcome at the highest reasonable cost they can conscience.
The economists call this “supplier-induced demand.” You might call it a nightmare.
In theory, this aligns payment with work done. In practice, it creates an incentive structure of almost breathtaking perversity. The system’s KPI is not “patient wellness” or “positive health outcomes.” It is “activity.” The business thrives not on health, but on sickness, and specifically, on the treatment of sickness:
More tests? More revenue.
More procedures? More revenue.
Longer stays? More revenue.
That surgery you might not need? Definitely more revenue.
You might say, “But doctors have ethics!” And they do. But they also have compensation plans.
The doctor isn’t evil. The doctor is just trapped in a system where “doing more” is financially rewarded and “doing less” looks like underperformance. If the hospital spent ₹80 crore on a CT scanner and it’s sitting idle, someone in the finance department is asking why. The doctor, consciously or not, becomes the solution to that problem.
And that’s before we even get to the Estimate Desk.

Many hospitals operate an “estimate desk,” which is a polite term for a bespoke price discovery unit that operates at the point of maximum emotional leverage. When a patient arrives, typically in an emergency with zero bargaining power, the desk provides an “estimate.”
This estimate is not a function of the medical procedure alone. It is dynamically priced based on real-time data signals of the customer’s ability to pay.
Wearing a Rolex? Estimate ↑
Arrived in a Mercedes? Estimate ↑
Mentioned insurance? Estimate ↑↑ (hospital knows insurer will negotiate, so start high)
Address in a wealthy neighbourhood? Estimate ↑
This is textbook price discrimination, the kind of yield management airlines use for seats. Except the variable isn’t your travel flexibility; it’s your desperation to see a loved one survive.
In India, to run anything other than a “pay-per-procedure” model, you need a pool of insured lives large enough to make the actuarial tables look like a plan rather than a random number generator. If only 40% of your patients have insurance, you aren’t “managing the long-term health of a population.” You are just running a retail shop where people show up when they are already broken.
In a market where 60% of customers are paying cash, the hospital has no incentive to keep you healthy and every incentive to make sure you pay your bill before you leave. But even if everyone had insurance, you’d still run into the Capex Doom Loop.

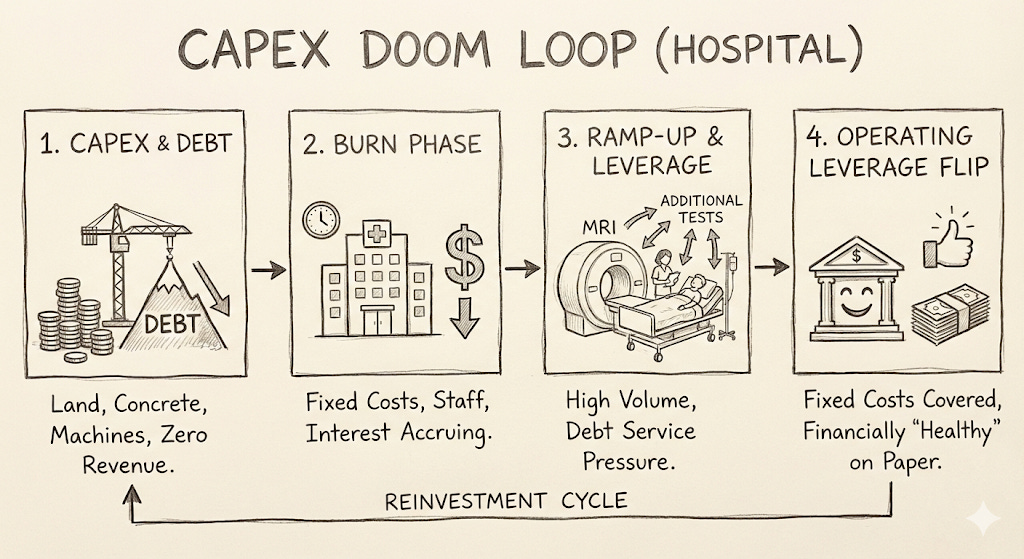
The financial life of a hospital begins with a very long period of spending money you don’t have on things that don’t yet work. You spend years pouring capital into land and concrete and machines that cost more than small islands.
During this phase, you have zero revenue, but you have a mountain of debt that is accruing interest with terrifying discipline. Debt, unlike patients, never misses an appointment.
By the time you actually open the doors, you are already in a deep financial hole. You have to hire a full staff of surgeons and nurses and keep the lights on in the ICU, regardless of whether there is anyone actually in the beds. This is the “burn” phase, where the hospital is a building of fixed costs and the only thing being utilised is the bank’s patience. Your lenders begin asking very reasonable, very pointed questions about when exactly this project is going to stop being a theoretical exercise in architecture and start being a business.
This is where the math of “operating leverage” becomes the hospital’s best friend and the patient’s most expensive problem. In the ramp-up years, the hospital is still gasping under the weight of its debt service. Every additional MRI, every extra night in the ICU, and every “thorough” metabolic panel is a contribution to the interest payment.
Eventually, if you get enough people through the door, the leverage flips. The fixed costs are covered, the bank is happy, and the hospital finally looks financially healthy on paper. It’s just that getting “healthy” on paper usually involves a lot of people getting a lot of tests they probably didn’t need.
This where the doctor’s principal-agent problem and the hospital’s debt repayment schedule fuse into a single economic machine. The hospital needs volume to service its debt. The doctor needs to hit revenue targets to keep their compensation. The patient needs care. Only one of these three parties has the information asymmetry to make it all work, and it’s not the patient.
If you are a health insurer in India, you are watching this happen from the other end of a very long, very expensive assembly line. In a fragmented network of thousands of hospitals, you are just a check-writer. You can’t stop the doctor from ordering the MRI. You can’t influence the care pathway. You are just standing there, trying to figure out how to pay as little as possible for a process you don’t control.
On paper, your industry is booming. In reality, you are trapped in an inflationary spiral where the growth is coming from the size of the invoices, not the number of customers.
To understand why this is happening, you have to look at the two different buckets of the business: Group and Retail.
Group insurance is what your HR department buys in bulk for 10,000 employees. In 2020, the regulator introduced a mandate requiring all employers to provide group health coverage. This was “forced adoption” for 150 million formal-sector workers. It was supposed to be the moment the industry finally achieved the scale needed to make the math work.
Instead, it acted as a massive dinner bell for the cathedrals of healthcare: the hospitals.

When you inject 150 million people into a healthcare system with “company money” in their pockets, hospitals react the way anyone with a mortgage and a monopoly reacts: they stop worrying about price. In the old world, where patients paid out-of-pocket, hospitals had to be somewhat sensitive to what a middle-class family could afford. In the new world, the “Payer” is a faceless corporation. Price sensitivity evaporated, and hospitals began raising procedure costs to service their massive debt.
The doctor, meanwhile, stopped being the gatekeeper of medical necessity and became the facilitator of billing. When the patient isn’t paying, the doctor doesn’t have to justify the third blood test or the “precautionary” specialist consultation. The insurance company is paying, the hospital’s revenue per patient is climbing, and the doctor’s commission is looking very healthy. Everyone wins, except the system itself.
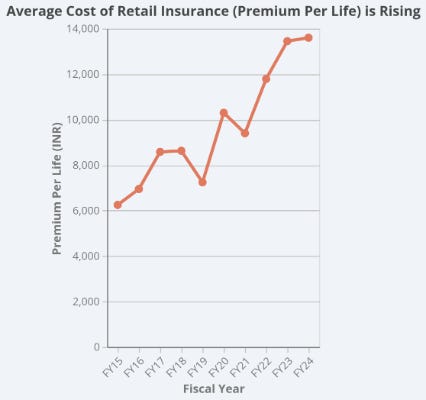
On the other hand, retail insurance is what you buy for your family at the kitchen table because you’ve realised that life is fragile and your savings account is thin. Because insurers don’t control the hospitals, they have to pass those rising “Group-driven” costs back to the only people they can: the policyholders.
The numbers tell the story of this hollowing out. Over the last decade, total premiums in the retail market have grown 5x, but the number of lives covered has only grown 2.5x. If your revenue is up 500% but your customer base is only up 250%, you haven’t “democratised” the product, you have just made it exponentially more expensive for the people who already had it.
This triggers a classic Adverse Selection Death Spiral. As premiums rise to cover medical inflation, the healthy retail customers, the ones who don’t expect to get sick, decide the price is too high and drop their policies. This leaves behind a pool that is sicker, older, and more expensive. That, in turn, justifies the next premium hike, which pushes out the next layer of healthy people.
The result is a system that isn’t expanding as much as it is getting heavier. The “premium per life” is going parabolic because the industry has moved from a “growth business” to a “cost-recovery business.” Standalone insurers are now price-takers in a market where they have no control over the actual product (healthcare).
Since they can’t control the cost of care, they have pivoted to a new business called friction engineering.
India’s leading insurers have managed to keep their claims ratios at 60-65%, but they haven’t done it by making healthcare cheaper but by making it harder to get. Claims rejection rates now average 10-14%.
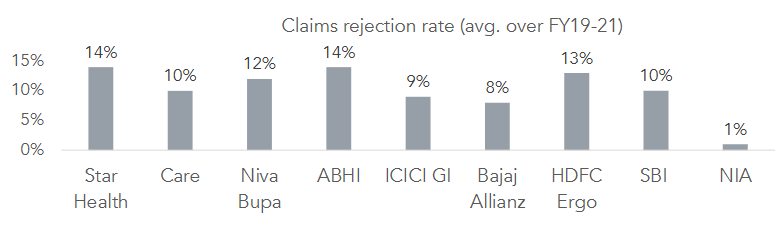
This creates a high-churn, high-unhappiness trap where the rational choice is wanting to switch their insurer. But they can’t switch, because if they’re sick, the next insurer will exclude their “pre-existing condition”. You are trapped in a relationship with a company that makes money by saying “no” to you.
This tension eventually turned into an actual war. In September 2025, the major insurers (Star Health, Tata AIG) ended “cashless settlement” at Max Hospitals, one of India’s elite chains. The insurers accused the hospital of overbilling and naturally, the hospital accused the insurers of underpaying.
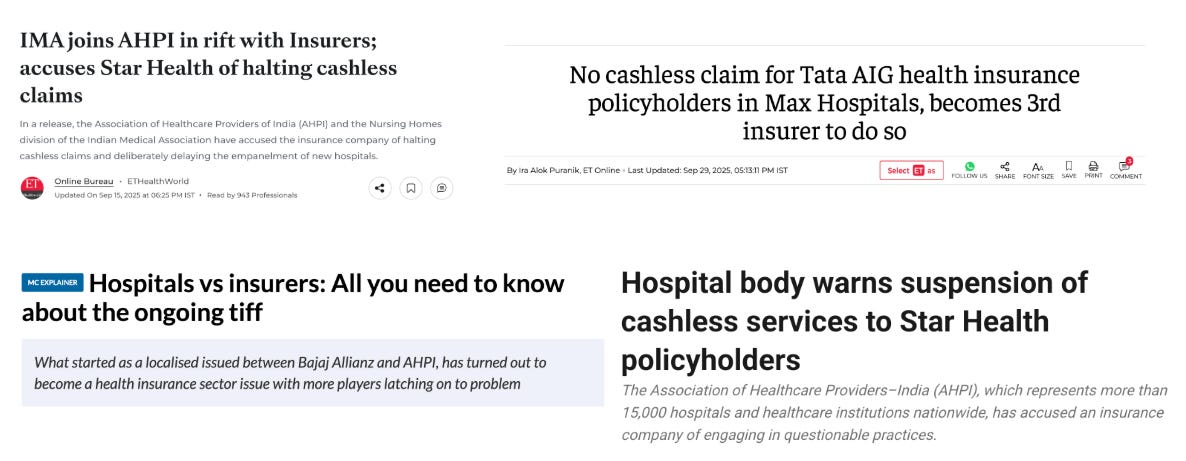
The patients, who had paid their premiums precisely so they wouldn’t have to worry about this, were told they had to pay out of pocket and “file for reimbursement later.” This is what happens when the “friction engineering” of insurance hits the “physical reality” of a hospital’s debt schedule and a doctor who is measured on how many patients they admitted today.
The fundamental problem is that no one controls utilisation. The doctor is supposed to, but the doctor is paid to do more. The hospital wants the doctor to do more. The insurer wants the doctor to do less, but the insurer doesn’t employ the doctor. Ultimately, the standalone insurer is a price-taker. When a hospital chain hikes procedure prices by 12%, the insurer has two choices: absorb it (hurting margins) or reject it (hurting customers).
Currently, they are choosing to hurt customers.
If you zoom out far enough, what the Indian healthcare system has built is a remarkably efficient luck-sorting machine. If you are lucky enough to live in a major city, lucky enough to have insurance that actually pays, lucky enough to work for a company with good group coverage, lucky enough to have an acquaintance who knows how to navigate a hospital - you get reasonable care. If you are unlucky in any of these dimensions, you get the other version.

The system isn’t cruel. It’s indifferent. And indifference, at scale, is its own kind of cruelty.
Someone had to decide that was unacceptable. Someone who had learned, young, what luck actually meant in a hospital.
[VI] The Company
How do you remove luck from the business of staying alive?
How do you remove luck from the business of staying alive?
If you are seventeen years old and watching your uncle die of pancreatic cancer, you might expect to learn something about biology or the limits of modern medicine. But if your father is a consultant for the NHS who can navigate the bureaucracy, coordinate the specialists, and pay for the procedures, you mostly learn something about circumstance.
Mayank Banerjee’s bauji, his paternal uncle, the person he was among the closest to in his extended family, was diagnosed with pancreatic cancer when Mayank was thirteen. He died four years later. It was the only time in his life Mayank cried. But what stayed with him wasn’t just the grief. It was the unfairness of it all.
His father, an ENT consultant who had moved the family from Agra to the UK for an NHS posting, could do things that a normal Indian family couldn’t. He knew which specialists to call. He knew how to read a treatment plan and push back on it. He could absorb costs that would have bankrupted most. The uncle got four more years partly because of medicine and partly because of who his brother happened to be. Without that accident of family, the outcome would have been different. The care would have been different. The timeline would have been shorter.
“The world is unfair and based a lot on luck,” Mayank says. “How do we remove the element of luck when it comes to the welfare of the people we love?”
This is the question Even is actually trying to answer. Everything else — the insurance structures, the hospital economics, the capitation contracts — is downstream of this.
How to Save Democracy (And Why Nobody Wanted You To)
Mayank followed the standard trajectory for people who are destined to either solve global problems or become deeply frustrated trying. He went to Oxford on a PPE degree, became president of The Student Union - a platform famous for producing a disproportionate number of British prime ministers - and found himself in rooms with people who ran things.
What he eventually realised was that the policymakers of the world were trying to keep old, creaky systems from falling over. The entrepreneurs and tech founders, on the other hand, were building new ones. While at the Union, he met founders like Eric Schmidt and Jack Dorsey, and found them more impressive than anyone in government or policy. What hammered home his epiphany was realising that, a century ago, someone with his credentials would have been expected to go out and run a country. Now, they become investment bankers and consultants. Mayank decided to drop out and started a company instead.

His first company, built with Matilde ‘Mati’ Giglio, a close friend he’d met at Oxford, was called Compass News. The premise: young people were making bad political decisions because they were poorly informed. The solution: machine learning that curated better news feeds. The logic was airtight. The only flaw was that young people, it turned out, did not particularly want to be better informed.
It was, as Mayank would later describe it, a vitamin masquerading as a painkiller. Nobody was sick enough to take it.
They decided to move on to other pursuits. Mati moved into venture capital. Mayank, restless and back to square one, returned to India looking for ways to be useful.
Fixing The Bill
The real moment of conception for Even is hard to pinpoint because there wasn’t a single eureka moment. There was a decade of accumulating dots — a close uncle passing away, a rejected YC application, a pandemic, a cold email to a then-stranger in Mumbai — that eventually cohered into something concrete.
When Mayank moved back to India on New Year’s Eve 2018, he brought a list of problems he wanted to examine further. If you are a normal person and you see a country with “massive structural problems,” you might think about moving to a nice, quiet suburb in Switzerland instead. But if you are an entrepreneur, that massive structural problem becomes an invitation.
The logic here is a form of the ‘Venture Capitalist’s Prayer’: scale compounds solutions the same way it compounds problems. If you can find a way to fix something for one person in India, you have a statistical head start on fixing it for a billion more.
Two problems on Mayank’s list kept bubbling to the top. The first was healthcare: the fact that 55 million Indians are pushed below the poverty line every year because they had the audacity to get sick. The second was whether India’s “demographic dividend” — the polite way of saying “a terrifyingly large number of young people who need to be productive” — would actually pay out, or if it would just be a demographic liability. He could not quite figure out a sustainable solution for the latter.
So he started with healthcare. And he called Mati.
She didn’t need much convincing. During her time in VC, she’d spent a considerable amount of time pondering over the elegance of the Kaiser Permanente model. She subsequently developed a thesis that a managed care company built for India could become one of the largest businesses in the world. For the second time in a row, it appeared they saw the world in a similar light. The only problem: neither had the technical chops to put this idea into motion.
That problem had a convenient solution. Mati had known Alessandro Ialongo since they were nine years old. Ale, as he was known, was three years into a machine learning PhD at Cambridge, and growing restless. He had interned at DeepMind, where the work was technically sophisticated but largely disconnected from anything that would change a person’s life in a measurable way — predicting wind farm output to balance energy loads, that sort of thing. He had begun looking for something more real.
Back in December 2018 — around the same time Mayank was landing in Delhi — Ale had been at NeurIPS when a document landed in his inbox from Mayank and Mati: an analysis of problems and opportunities in the Indian market. He read it, found it interesting, and filed it away.
The more interesting conversation came later. By early 2019, Ale was thinking seriously about what came after the PhD. He had seen enough of DeepMind and enough of other domains — fintech, energy, healthcare — to have a view. Healthcare, he thought, was where the asymmetry was most extreme. Fintech had already been transformed by software. Healthcare hadn’t. Reducing the marginal cost of a service far enough changes consumption entirely; demand that was constrained by price suddenly wouldn’t be. The ingredients for transformation were there. Nobody had combined them correctly.
Through 2019 and into 2020, the three of them began talking more seriously. Then the pandemic arrived.
Ale was at the Max Planck Institute, nominally finishing his PhD, when the lockdowns hit. The benchmarks he was optimising felt increasingly abstract while the world outside was visibly falling apart. He and Mayank started calling almost daily — mapping the problem space, discarding ideas, coming back to healthcare.
They spoke of better underwriting through AI. Standardising costs. Predicting readmission. Mati was less involved at this stage, stretched thin by her VC work. But the daily calls between Mayank and Ale eventually landed on something specific: a fully comprehensive membership covering care across Bangalore. The insight was the OPD gap — Indian health insurance almost universally covered hospitalisation and almost universally didn’t cover outpatient care: the doctor visits, diagnostics, and prescriptions that constitute the majority of actual healthcare interactions. Their product would cover everything. If the doctor said it was needed, it was covered.
In the meantime, they made the traditional opening move for founders in the 21st century: applying to Y Combinator.
It turns out that if you tell a committee in San Francisco that you want to fix a broken, multi-decade, colonial-era medical system in a country they’ve mostly seen in PowerPoint slides, they might be a little skeptical.
They rejected the application. In the world of startups, getting rejected by YC is a standard part of the origin story, right up there with “hiring your father” and “cold-emailing people who are much more successful than you” — both of which Mayank would eventually do. The team came to Bangalore for the interview anyway, which is where they met Viren Shetty.
Viren ran Narayana Health, which had spent three decades figuring out how to deliver cardiac surgery at a price ordinary Indians can afford. Working with his team, Mayank and Mati’s first idea was simple to the point of seeming obvious: give patients a fixed price for procedures. In almost every other market, you know what something costs before you buy it. In Indian hospitals, the final bill is a surprise. They wanted to eliminate the surprise.
The math was tractable. A procedure costs ₹3 lakhs. Three percent of the time, complications push it to ₹5 lakhs. With enough actuarial data, you could price a guaranteed fixed rate that absorbed the variance and still made money. It was insurance wearing a different hat.
Through this work they were introduced to Animesh Roy — then a hospital operator at Narayana with seven years of experience. Viren, characteristically generous, made the introduction without making a fuss about losing someone good. Animesh would go on to become Even’s first critical hire, the person who knew how hospitals actually worked from the inside.
The pandemic arrived. The fixed-price idea stalled. But the relationships held.
The trio — Mayank, Mati, and Ale — became convinced not just that the model was fixable, but that if it was fixed correctly, this could become one of the largest companies in the world. Ale moved to India on the 1st of February. They set up shop in Bangalore.

How much ignorance is optimal?
If you were to design a team to disrupt a multi-billion dollar, highly regulated, capital-intensive industry in the world’s most populous country, you might look for people with thirty years of seniority and deep, jagged scars from the system. You probably wouldn’t look for a PPE student, a venture capitalist, and a PhD in deep learning.
Even’s founding team were, by any reasonable standard, a group of misfits -unmistakably round pegs in square holes. Mayank Banerjee had studied politics. Matilde Giglio had worked in venture. Alessandro Ialongo was a machine learning researcher at DeepMind. Between them, they had exactly zero experience running a hospital or calculating the “Loss Development Triangle” of a health insurance book.
To fix this, they had to bring in some operational leadership. Animesh Roy joined as the Head of Healthcare Operations (He has since been promoted to CEO of Even Hospitals). Now that they had someone who grokked hospitals, they went after the hardest part of the business: the actuarial table.
You cannot run an insurance company if you don’t know how to price the probability of 100,000 different people having 10,000 different medical problems. Mayank cold-emailed Raunak Jha, who had been the Chief Actuary at several of India’s top insurers. She gave him the classic “let’s grab coffee next time you’re in Mumbai” that lives comfortably in the future tense. Mayank, who was in Bangalore, immediately replied that he just happened to be flying to Mumbai this Friday. He wasn’t, of course - he booked the flight anyway.

This is the classic “Entrepreneurial Arbitrage” move: you trade a ₹5,000 flight ticket for the chance to pitch an actuary on a dream. It worked. He flew down, explained the math of integrated care, and convinced her to leave the safety of the incumbents to become the CRO and CFO of a startup. To round out the circle, Mayank’s sister Ira joined from Oxford.
By the time Khosla Ventures wrote the seed check, the team consisted of four people who knew nothing about healthcare and two people who knew almost everything. This is a very efficient ratio. If you have too many insiders, you spend all your time explaining why things can’t change. If you have too many outsiders, you spend all your time figuring things out. Even found the sweet spot: they had just enough ignorance to try something radical, and just enough expertise to make sure it actually cleared the regulator (or so they thought).

Really Rethinking Health Insurance
In June 2019, the founding team at Even sat down to write what they thought would be a straightforward investment thesis. The document was titled “Rethinking health insurance in the developing world and the case for an Oscar for India.”
Oscar Health, for context, was the American Insurtech that had spent the previous decade trying to prove that health insurance didn’t have to be a miserable experience. Founded in 2012 by Josh Kushner and Mario Schlosser, Oscar built a consumer-grade interface on top of the notoriously hostile American insurance system - better app, simpler claims, concierge doctors, human customer service. It was a technology company wearing an insurance company’s clothes, and it had raised over a billion dollars on the promise that fixing the customer experience was the first step to fixing the economics.
Even’s thesis to replicate Oscar’s playbook was objectively beautiful. India had a billion uninsured people and a market growing at 30% annually. But the really exciting part, if you are a fan of structural inefficiency, was the 58% claims ratio.
In the insurance business, if your claims ratio is 58%, it means you are collecting ₹100 in premiums and only paying out ₹58 for actual medical care. In the United States, this is effectively illegal; if an insurer’s ratio drops below 80%, they are legally required to mail the customers a refund check for being so aggressively overcharged. In India, a 58% ratio was just called “a Tuesday.” It was a magnificent way to be an insurance company, provided you didn’t mind that your customers felt like they were participating in a very expensive prank.
The opportunity was obvious: build Oscar for India.

To understand better what this means, consider the plan in two parts:
Part 1: Bring Indian Insurance customer experience on par with the West
Offer comprehensive coverage (not just hospitalisation, but ongoing medications and preventive care)
Bypass agent-based distribution (save the 12% commission that incumbents paid to middlemen)
Simplify the claims process (approve more than the 58% industry standard)
Part 2: The differentiated insight
Make health data sharing mandatory in exchange for cheaper premiums
Issue fitness trackers to all policyholders
Link usage data directly to premiums - more data shared, lower costs
Create positive selection bias (healthy people join for savings, creating a virtuous cycle)
The document concluded: “India is the ideal starting point for a land and expand strategy across the developing world. If a new entrant is able to link coverage to the exchange of first party health data, not only could it provide a competitive moat, but it completely rethinks the fundamental incentives at play in the market.”
It was a tech-first vision. Data would solve everything. Wearables would align incentives. Consumers would trade privacy for savings. The model would start in India and expand globally.
Reading it now, with the benefit of hindsight, the document is fascinating for what it got right and what it completely missed.
The wearables idea never got far enough to properly fail. It got far enough to reveal, fairly quickly, that it was solving the wrong problem. The insight it was built on - that aligning member incentives would fix healthcare costs - was directionally correct but aimed at the wrong target.
“The easy part is to tell your patients to do something, the hard part is to actually get them to do it and follow up on whether they have actually done it. “- Mayank Banerjee
If you offer someone a 5% discount to walk 10,000 steps, the person who was already walking will take the money. The person who prefers sitting on the couch and eating a samosa will continue to do so, because the marginal utility of the samosa is significantly higher than the marginal utility of the five-dollar discount. You end up paying healthy people to stay healthy, which is nice, but you don’t actually change the risk profile of the people who might actually cost you money.
More importantly, the Even team discovered that you cannot solve a Principal-Agent problem with a wristwatch. Even if your member is walking 15,000 steps a day, they still eventually have to go to a hospital. A Fitbit can tell you how many calories you burned, but it cannot stop a hospital from running a utilisation play on your tension headache.
The team moved on quickly, and the speed with which they abandoned the wearables thesis turned out to be one of their better early decisions.
In November 2021, launched their first product: a hospital membership programme usable across major networks like Narayana Health, Aster and Fortis. You pre-paid for care and got a card. No claims. No friction. Just show your card and receive treatment.

The seed round that funded that launch was $5 million, led by Khosla Ventures in July 2021, and the co-investors on the cap table were unusual enough to deserve attention. Founders Fund and Lachy Groom came in alongside Nikesh Arora of Palo Alto Networks, Kunal Shah of CRED, Nithin Kamath of Zerodha, and Tom Stafford of DST Global. This wasn’t a healthcare specialist round.
It was a collection of people who had each built or backed category-defining businesses in their respective domains - cybersecurity, consumer fintech, retail investing, global technology - and had each independently concluded that Even was attempting something in the same category of ambition.
At the seed stage, Even had no proven product, no regulatory clarity, and no demonstrated unit economics. What they had was a thesis and a team. That this specific group of people decided the thesis was right, before any of the proof existed, is worth keeping in mind as the proof accumulates.
The Regulator Knocks
Four months later, the Insurance Regulatory and Development Authority of India (IRDAI) issued a memo. It essentially said: “We noticed you are calling this a ‘membership,’ but we are looking at the part where you take money to cover the medical risk of your users. That is insurance. We have very expensive rules about that. Please stop.”
In the world of financial regulation, if it looks like a duck and quacks like a duck, the regulator will fine you for not having a duck-operating license.
Then came the death knell. In April 2022, the Insurance Regulatory and Development Authority of India (IRDAI) looked at Even’s “membership” product and decided to delete it. Even was directed to stop selling immediately and refund every single customer. Months of building evaporated in a single afternoon.

There is a specific kind of silence that follows a moment like this. The kind where you sit with the wreckage and try to figure out if the thing you just lost was the wrong version of the right idea, or just the wrong idea.
For Even, the answer came quickly. The regulator hadn’t killed their vision; it had simply revealed what Even needed to become.
So, they went back to first principles, got properly licensed, and rebuilt, this time with the regulator in the room rather than knocking on the door.
The Second Coming
Even relaunched in October 2022, but this time the regulator was “in the loop.” They became a licensed corporate agent, managing lives for other insurers.

Here’s where it gets clever, and where most people get confused.
Even is not a licensed insurance company. They don’t have an insurance license from IRDAI. They don’t carry the massive solvency capital (hundreds of crores) required to underwrite risk directly.
Instead, Even operates as a Corporate Agent for licensed insurance carriers. Under current IRDAI regulations, a Corporate Agent is an entity licensed to distribute insurance products on behalf of one or more insurance companies while the actual underwriting license and risk sit with its partner insurers.
Here’s how it works:
Even partners with a licensed insurer (let’s call them “Partner Insurance Co.”)
Partner Insurance Co. holds the regulatory license and provides the balance sheet to underwrite the insurance risk. They’re the entity that IRDAI regulates and they bear the ultimate financial risk.
Even acts as a Corporate Agent, which means they:
Acquire members (marketing, sales, distribution)
Operate the care delivery network (clinics, hospital)
Coordinate care and route patients through their network
Provide member service and support
Partner Insurance Co. pays Even a commission/fee (typically in the range of 10-30% of gross written premiums, though the exact structure varies by partnership) for distribution and care coordination services.
Even also captures the provider margin from the owned clinics and hospitals, which doesn’t flow through the insurance partnership at all, it’s just normal healthcare facility revenue from treating patients.
The carrier manages the formal insurance operations: underwriting, actuarial reserves, regulatory reporting, claims adjudication (though Even provides the care delivery data that informs these decisions)
Why this structure?
Capital efficiency: Even doesn’t need to raise ₹100+ crores in solvency capital to get an insurance license. The partner provides that.
Speed: Getting an IRDAI license takes years and requires proving insurance expertise. Becoming a Corporate Agent is faster and lets Even focus on what they’re actually building: integrated care delivery.
Focus: Even can concentrate on care delivery, member experience, and utilization management, their actual competitive advantage, while the partner handles regulatory compliance, actuarial reserving, and insurance back-office operation
The trade-off:
Even gives up some economics. If they owned a full insurance license, they’d keep 100% of the underwriting profit. As a Corporate Agent, they get a commission and have to share the insurance economics with the partner carrier.
They also have less control over certain insurance operations (final underwriting decisions, pricing flexibility, reserve management) since those sit with the licensed carrier.
But they get to operate much faster with much less capital and can scale the care delivery network (which is where their real competitive advantage lies) without the regulatory burden and capital intensity of becoming a full insurer.
In November 2022, one month after relaunching with the new structure, Even raised a $15 million Series A round. Alpha Wave and Lightrock (via Aspada) led the round, with Khosla Ventures, Founders Fund, Kunal Shah, and Tom Stafford all following on from the seed.
The timing is the most important thing about this round. Even had just been shut down by the regulator, forced to refund every customer, and required to rebuild their entire product architecture from scratch.
They raised $15 million in that condition - not despite the shutdown but, in a meaningful sense, because of what they did after it. The shutdown had handed them a precise diagnosis of exactly what they needed to become. The Series A investors weren’t backing a company that had avoided a near-death experience.
They were backing a company that had walked through one and come out with a cleaner model, a licensed structure, and a clearer understanding of the problem they were actually solving. The capital was allocated to scaling the clinical team and building out preventive care programmes for diabetes, PCOS, and obesity - the chronic disease layer that would eventually make the insurance economics work.

By now, Even had the licensed products. They had insurance relationships. They were empaneled with major hospital networks across India. They were coordinating care through technology, routing patients to quality providers, and managing the member experience from end-to-end.
On a pitch deck, the model was flawless.
A member gets sick. Even’s telehealth doctors triage them. If it’s something minor, it’s handled over the phone. If it’s serious, the member is routed to a high-quality partner hospital. Even manages the claims process to ensure smooth reimbursement. The member gets better care, the hospital gets a reliable payer, and the insurer gets a managed loss ratio. Everyone wins.
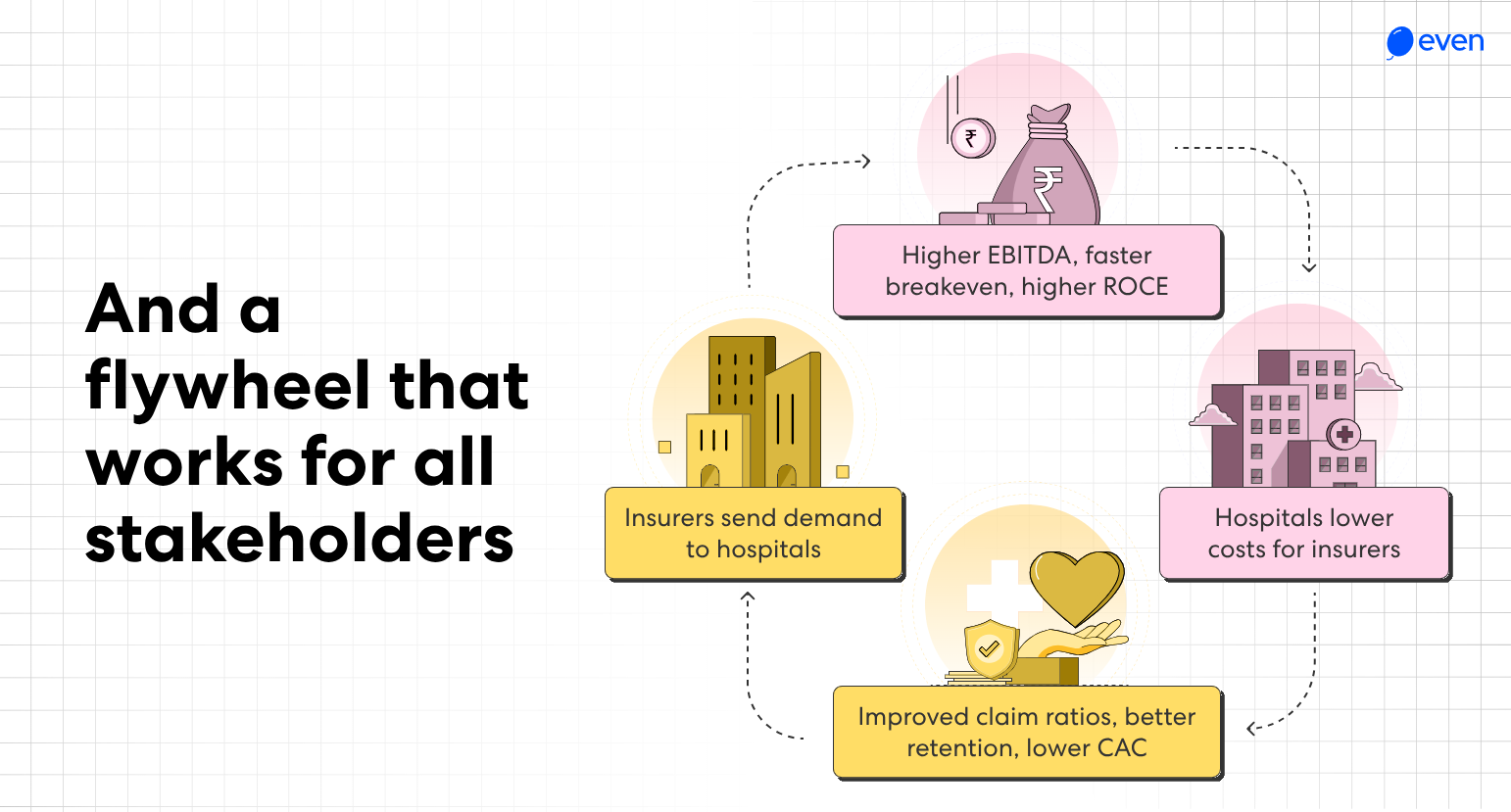
That’s when they discovered the actual problem.
The Headache MRI problem
Every Even member who walked into a particular reputable private hospital with a tension headache, the kind you get from looking at a monitor for twelve hours (*nervous laughter*), came out with ₹20,000 in diagnostic tests. Not occasionally. Not a few outliers. Every single one.
Even had discovered the principal-agent problem in its purest form. The doctor wasn’t their agent. The doctor was on the hospital’s payroll. And the hospital’s economics made this inevitable. To understand why fixing this requires owning both sides of the transaction, you need to see where the money actually flows in this system.
Why Everyone Is Getting Rich Except the People Paying the Bills
In the Hospital Business, if a patient pays ₹100, the hospital spends about ₹75-80 to deliver the care and keeps ₹20-25 as EBITDA. That is a very healthy 25% margin.
In the Insurance Business, if a patient pays ₹100 in premium, the insurer pays out roughly ₹100 (or more) in claims and another ₹15 in operations. The EBITDA margin is somewhere between -5% and +5%.
The provider’s profit pool is ten times larger than the insurer’s profit pool.
The person who owns the concrete and the doctors has all the leverage. The person writing the checks is just a passenger.
This was the system Even Healthcare walked into in 2019. They thought the answer was “better insurance.” They quickly learned that if you are an insurer who doesn’t control the care, you aren’t really in the insurance business. You are just an unpaid collections agent for a hospital.
[VII] The Model(s)
Surely, Someone Has Figured It Out?
If you are an insurance company and you realise that you are barely breaking even while the hospital you pay is making a 25% margin, you eventually have a very simple, very expensive thought: “I should probably stop being the person who writes the checks and start being the person who receives them.”
In Silicon Valley, when you realise that the customer experience is terrible because the value chain is fragmented and nobody has enough leverage to fix the broken parts, you call the solution “Vertical Integration”
In 2017, Keith Rabois crystallised a pattern that explained the most durable companies of the previous decade:
This pattern has created iconic companies:
Opendoor took fragmented real estate (NPS ~30) and vertically integrated the home-selling process
Faire took wholesale commerce (NPS ~25) and built end-to-end control over discovery, ordering, and fulfillment
Amazon vertically integrated retail, logistics, and payments when e-commerce was a mess
The pattern repeats: large market, terrible customer experience, fragmentation preventing improvement, vertical integration to control the full value chain, simplified product that works.
Indian healthcare fits this pattern:
Large market: $250B by 2030 (Was around $105B in 2022)
Highly fragmented: 15,000+ empaneled hospitals. No single entity controls >2% of capacity
Low NPS: Insurers at 40-50, hospitals at 40-50
Broken value proposition: IPD-only coverage, claim denials, platform wars
The vertical integration answer in healthcare is called a Payvidor. And while that sounds like something a McKinsey consultant would come up with after having three martinis, it is very much real and is very much proven.
It is a portmanteau of Payer (the insurer) and Provider (the care delivery). The strategic insight is that if you own both sides of the ledger, you can internalise the adversarial relationship. You stop fighting over the ₹25 margin and you just... keep it. More importantly, you align the incentives so that the most profitable thing for the company is also the thing that keeps the patient from getting sick.
This isn’t a new idea. It is a proven, multi-decade trade that has worked in almost every geography where someone was brave enough to try it.
Global Precedents
Let’s start with the gold standard, a company so iconic that Even proudly confirms that their vision is akin to building the ‘Kaiser for India’.

Kaiser Permanente is the integrated healthcare model that inspired everything that came after. Founded in 1945 by industrialist Henry J. Kaiser and physician Sidney Garfield, it began as a health plan for Kaiser’s shipyard workers during World War II. The insight was simple: if you’re going to insure workers, you might as well own the hospitals and doctors too, so you can control costs by keeping them healthy rather than just paying bills when they get sick.
Today, Kaiser operates primarily in California and a handful of other western states. They have 12.7 million members and $95 billion in revenue. On paper, their operating margins look low, around 2% to 4%. In reality, that’s what happens when you own the entire stack: the profit that would normally accrue to insurers, hospital chains, and specialist groups is captured internally instead of showing up in any single line item.
Kaiser works because they solved the “Headache MRI” problem by changing how the doctor gets paid. A Kaiser doctor is on a salary. Rather than being measured by volume of care, they are measured by outcomes. If a Kaiser primary care physician prevents a diabetic from being hospitalised by managing their medication correctly, Kaiser saves a few thousand dollars in claims. And instead of losing on commission income, they get a bonus for being a good doctor.
When you own the insurance risk and the doctor’s time, prevention becomes a profit-maximizing strategy.
The only problem with the Kaiser model is that it took seventy-five years and $50 billion in capital to build. They own 40 hospitals, 37 of which are in California alone. For a long time, the consensus was that being a Payvidor was a great business that required you to be a sovereign wealth fund with a century-long time horizon.

Then UnitedHealth’s Optum division showed up and proved that you don’t actually need to own the concrete to control the care.
Optum is the healthcare services arm of UnitedHealth Group, the largest health insurer in the United States. Starting in the early 2000s, UnitedHealth realized that simply paying claims was a terrible business, they were hostages to hospital pricing with no control over utilization. So, they began buying up physician practices, starting with primary care groups and eventually expanding to specialists, surgery centers, and urgent care clinics.
By 2024, Optum had become a $253 billion revenue monster, larger than many Fortune 100 companies, and they didn’t build a single hospital from scratch.

The strategic insight here is to own the control layer.
Instead of pursuing a multi-billion-dollar hospital buildout, Optum just bought the primary care practices. They employ 70,000 physicians who act as the “gatekeeping layer.” When you get sick, you see an Optum doctor. That doctor decides if you need a specialist, if you need an MRI, or if you can just be managed at home. Optum contracts with external hospitals for the big surgeries, but because they own the doctor who makes the referral, they control the utilization.
They get the Kaiser-level outcomes, with the majority of cases resolved in primary care thus enabling lower costs and higher patient satisfaction, without the capital intensity of owning a building with a mortgage.
If you want to know what this looks like in a place that actually resembles India, you look at Hapvida NotreDame in Brazil.
Hapvida was founded in 1979 in Fortaleza, a mid-sized city in Brazil’s northeast, far from the wealthy urban centers of São Paulo and Rio. The company started with a simple thesis: Brazil’s government health system was broken, the emerging middle class wanted private care, but traditional insurers were expensive and delivered terrible experiences. The solution was vertical integration, own the clinics and hospitals, employ the doctors, and cut out the middlemen.

Over four decades, Hapvida expanded methodically across Brazil, acquiring competitors and building out its own network. In 2020, they merged with NotreDame Intermédica, another major integrated player, creating the largest healthcare operator in Latin America with 15 million beneficiaries.
Brazil has exactly the same problems India does: fragmented hospitals, low insurance penetration, and a growing middle class that is tired of the government’s broken promises.
Across all these models, three principles emerge:
Primary care is the chokepoint: If you don’t control the first doctor the patient sees, you don’t control the bill. Control the entry point and you control 85% of the decisions.
Employment beats contracts: You can’t “align incentives” with a third-party hospital that has its own debt to pay. You have to employ the doctor. You want the person in the white coat to care about the patient’s health, not the hospital’s EBITDA.
Capital intensity is a choice: You don’t have to build a $50 billion network. You just have to own the parts of the value chain that drive the most cost.
The Salaried Doctor
By the summer 2023, Even had proven the insurance model worked. They had tens of thousands of members, solid retention numbers, and claims ratios that made traditional insurers look amateur. But they were still operating primarily as a telehealth-first company. Members called when they were sick, talked to a doctor over video, got prescriptions sent to pharmacies, and only went to partner hospitals when things got serious.
This worked, but it had limits. Roughly 20% of medical issues genuinely require physical examination or in-person procedures. You can’t diagnose a skin condition reliably over video. You can’t do a blood draw remotely. You can’t examine a child’s ear infection through a phone screen.
For those cases, Even was routing members to partner clinics and diagnostic labs. Every referral meant paying external provider rates and losing control of the care experience.
The decision to build physical clinics was about internalising this 30% of care delivery they were currently outsourcing, capturing the provider margin, and controlling quality end-to-end.
But opening physical clinics meant solving a problem that had nothing to do with real estate or equipment: they needed to hire doctors. And the economics of how doctors get paid in India made that complicated.
The Specialist Compensation Model (And Why It’s Broken)
To understand what Even had to overcome, you need to understand how specialist doctors typically earn money in India’s private healthcare system.
A “specialist” in this context means any doctor beyond a general physician. This includes cardiologists, orthopedic surgeons, dermatologists, gynecologists, ENT specialists, pediatricians, any doctor with specialised training beyond basic MBBS (Bachelor of Medicine, Bachelor of Surgery).
Most specialists in India don’t work as salaried employees of a single hospital. Instead, they operate as independent contractors who split their time across multiple hospitals and may also run their own private clinics.
Even decided to blow that model up. They started hiring doctors as full-time, salaried employees. And because they were asking these doctors to leave the high-upside world of commission, they didn’t ask them to take a haircut. Instead, they gave them ESOPs over and above a competitive salary.

The message: “You’re not a commissioned sales agent anymore. You’re an owner. When Even succeeds because we keep members healthy and costs low, you benefit through equity upside.”
With that they turned the doctors into owners of the system rather than scavengers within it.
Mayank’s pitch was blunt: “You hate sales targets. We hate sales targets. Come work for us on a full-time, fixed salary. No commissions. Your only job is to keep the patient healthy.”

By removing the per-procedure bonus, Even solved the principal-agent problem at its source. The doctor no longer had a financial reason to find a “clinical concern” that required expensive diagnostic workup. If a patient’s tension headache could be managed with stress reduction and basic medication, the doctor prescribed exactly that, because their salary was the same either way, and their equity value increased when the company spent less on unnecessary care.
[VIII] Getting Going
The First Clinic
Normally, opening a primary care clinic is a brutal exercise in patience and cash burn.
The standard trajectory: You lease space, build out the clinic (₹40-60 lakhs in capex), hire doctors and staff, open the doors, and then... wait. You spend the first 6-12 months building awareness, relying on walk-ins and referrals to slowly build a patient base. You burn ₹10-15 lakhs monthly in operating costs while seeing maybe 5-10 patients a day. It typically takes 12-18 months to reach profitability, assuming you survive that long.
Even’s Indiranagar clinic reached profitability in three months.

How? Because Even already had the patients.
By mid-2023, Even had accumulated roughly 20,000 insurance members across Bangalore through their telehealth-first model. Members paid annual premiums and accessed care primarily through video consultations.
When members called Even’s telehealth line with health concerns, the salaried doctors triaged them:
60-70% of cases could be handled completely over video (prescription sent digitally, follow-up scheduled by phone)
30-40% of cases needed in-person care (physical examination, diagnostic tests, procedures)
Before the clinics existed, that 20% got routed to partner facilities. Even paid external provider rates and lost control of the experience.
Once the Indiranagar clinic opened, the telehealth doctors simply started routing that 30-40% to the Even clinic instead. “You need a physical exam. Our clinic in Indiranagar is 2 kilometres from you. We have an appointment available this afternoon.”
The clinic didn’t open at full capacity overnight. Even deliberately drip-fed patient routing in the early weeks because they needed to know they could actually deliver care at the standard they’d promised before scaling it up. A bad experience for member 5000 is recoverable. A bad experience for member 50 becomes the story that travels through your entire member base before you’ve had a chance to fix it.
Once they were confident the care quality held, they opened the routing fully. Within three months, the clinic was profitable. Not because of walk-in traffic or marketing campaigns, but because Even had what you might call demand visibility - they already knew exactly how many members needed in-person care, where they lived, and what they needed.
Traditional clinics build supply and hope demand materialises. Even built demand first, then added supply precisely where their existing members needed it and turned the dial up only when they were sure the product was ready.

The Blood Test That Prints Money
Once Even had physical clinics operational, they discovered something that would reshape their entire economic model: in-house diagnostics aren’t just margin-positive, they’re wildly margin-positive.
In India, standalone diagnostic chains like Dr. Lal PathLabs and Thyrocare run 65-75% gross margin businesses. The math is almost absurd:
A comprehensive blood panel costs the patient ₹1,200. The marginal cost to the lab - reagents, consumables, technician time, electricity - is roughly ₹180-250. Contribution margin: ₹950-1,020 per test (79-85%).
An MRI scan costs the patient ₹4,000-6,000. The marginal cost to the facility - electricity, technician time, radiologist reading time - is roughly ₹400-600. Contribution margin: ₹3,400-5,600 per scan (85-93%).
Why such extreme margins? Because diagnostics have massive fixed costs (buying the equipment) but near-zero marginal costs (running one more test).
That ₹2 crore MRI machine costs the same whether you run 10 scans a day or 50 scans a day. Once you’ve amortised the equipment cost, every additional scan is almost pure profit. (Editor’s note: we actually wrote an essay on this topic in 2020. It contains some interesting facts about the margin structure and market dynamics of diagnostics businesses. Link below),

Even realised: if we’re already sending members to external labs and paying ₹1,200 per blood test, why not build the lab in-house, pay the ₹200 marginal cost, and keep the ₹1,000 margin?
They built basic diagnostics labs into their clinics. The economics shifted immediately:
Before (external lab):
Patient needs blood work
Even routes to partner lab
Lab charges Even ₹1,200
Even’s insurance pays ₹1,200
Even’s margin: ₹0
After (in-house lab):
Patient needs blood work
Doctor orders test at Even clinic
Lab processes test (marginal cost ₹200)
Even’s insurance “pays” Even’s lab ₹1,200 (internal accounting)
Even’s margin: ₹0 (still 0, Even passes this down as savings for the patient and the insurer)
Every blood test that moved in-house converted a ₹1,200 cost into ₹1,000 operational savings that directly flows to the patient and the insurer. At 10,000 tests monthly across multiple clinics, that’s ₹1 crore in monthly cost reduction that was previously leaving the system entirely.
They’d proven the clinic model worked. They’d internalised diagnostics. They’d hired salaried doctors and made the economics sustainable. What did the market pull out of them next?
What the Market Pulled Out of Them
The product evolution at Even followed a pattern you might call “Customer-Led Expansion.” It’s the story of a company that set clear boundaries about what it would and wouldn’t do, only to have customers systematically prove those boundaries were artificial.
The original plan, after the regulatory reset in 2022, was clear: “We are an insurance distributor that owns some primary care clinics. We handle routine checkups, chronic disease management, and basic diagnostics. For anything complex, specialty care, surgeries, hospital admissions, we partner with established hospital networks. Customers want trusted, brand-name institutions for the serious stuff.”
This made sense on paper. It was capital-efficient (no expensive hospital infrastructure), operationally focused (do one thing well), and aligned with customer expectations (nobody trusts a startup with brain surgery).
Then the data started revealing something different.
The first boundary to fall was specialty care.
The assumption: “Nobody will trust a two-year-old startup for dermatology. They’ll want to go to a branded dermatology clinic with 20 years of reputation.”
Even launched with partnered dermatologists, external specialists that members could see through the insurance network. But members kept asking: “Can I see a dermatologist at the Even clinic? I’m already there for my checkup, I trust my primary care doctor, can you just add dermatology?”
Even hired a dermatologist. Within three months, dermatology became one of their highest-volume specialties. Not because Even had built a world-class dermatology brand, but because members valued convenience and trust over brand heritage. If you already trust the clinic for your diabetes management, you trust them for your skin condition.
The lesson: The boundary between “primary care” and “specialty care” was permeable. Customers didn’t care about the distinction. They cared about integrated, convenient care from providers they’d already built relationships with.
The second boundary was pediatrics.
Parents are, for obvious reasons, the most protective and least price-sensitive customers in the world. The assumption was ironclad: “Parents will only take their children to dedicated children’s hospitals. They want pediatric specialists, child-friendly facilities, and established reputations.”
But parents, it turns out, are also exceptionally good at sensing when they’re being upsold. They’ve been through enough “precautionary tests” and “just to be safe” diagnostic batteries to recognise when a hospital is optimising for revenue rather than their child’s health.
When Even opened pediatric services at their clinics, parents flooded in. Not for complex cases, those still went to children’s specialty hospitals, but for the high-volume, routine needs: vaccinations, common illnesses, growth monitoring, minor injuries. The salaried pediatricians had no revenue targets to hit, no pressure to run a precautionary battery of tests on every sniffly child.
The value proposition wasn’t “we’re better pediatricians than the children’s hospital.” It was “we’re not trying to maximise your bill, and that matters more to you than fancy wall murals.”

And thus, Even hired pediatricians. Another boundary dissolved.
By late 2024, Even was in an unusual position. Their clinics were profitable. Their diagnostic labs were contributing healthy margins. Member retention was exceptional. The integrated primary care model was working.
But when they looked at where their insurance money was actually going, the total claims payouts across all members, they realized that 70% of total claims spending was flowing to external hospitals for routine surgical procedures.
Not complex tertiary care. Not rare diseases. Routine surgery: appendectomies, gallbladder removals, hernia repairs, C-sections, fracture repairs.
These aren’t unpredictable “black swan” events. They’re actuarially consistent. In any population of 50,000 members, roughly 4-5% will need routine surgery annually. That’s 2,000-2,500 procedures a year, occurring with clocklike regularity.
Every one of those surgeries sent to an external hospital meant two problems:
First, loss of care pathway control. The moment a member entered an external hospital, Even lost visibility and influence. A straightforward appendectomy could suddenly require five “precautionary” diagnostic tests, two extra observation days, and non-formulary medications. Even’s insurance was paying the bill, but they couldn’t control the utilization. The incentives were misaligned again: the hospital made more money if they did more things to the patient.
Second, margin leakage. The provider EBITDA margin on surgical procedures in India runs 20-25%. When Even sent members to external hospitals, that 25% margin went to the hospital. From Even’s perspective as the insurer, it was a cost. But if Even owned the operating room, that same 25% would be profit (or in true Even fashion, savings passed down to the customer).
By early 2024, Even’s leadership team looked at this dynamic and realized they were running a beautifully efficient patient acquisition and triage funnel - telehealth, clinics, diagnostics - that was ultimately feeding someone else’s revenue stream for the highest-margin procedures.
They had a choice:
Option A: Remain a Payer
Continue as a “care coordination layer.” Manage members, provide excellent primary care, coordinate with partner hospitals for surgeries and admissions. Write increasingly large checks to external hospitals that have every incentive to overcharge and over-treat.
Option B: Become a Provider
Build a hospital. Own the operating rooms. Internalise the 25% provider margin on routine surgeries. Control the full care pathway from telehealth triage through post-surgical recovery.
For most tech startups, Option B is where growth ambitions go to die. Building a hospital is capital-intensive (tens of crores), operationally complex (managing surgeons, nurses, medical equipment, compliance), and usually slow (typically 2-3 years from groundbreaking to operations).

But Even had been studying the structural economics of Indian healthcare infrastructure. And they’d realised something that changed the calculus entirely: in India, building a secondary care hospital isn’t actually that hard. It’s dramatically easier, faster, and cheaper than in developed markets.
“We had a model that worked across different hospitals... But we realized that we couldn’t change human behaviour through a tech platform alone.” - Mayank Banerjee
The question wasn’t “Can we operationally run a hospital?” (The answer was probably yes - hospitals are complex but not unknowable, and Even could and did hire experienced hospital administrators.)
The question was: “Can we make the unit economics work? Can we build and operate a 70-bed acute care facility with the capital typically reserved for a Series A SaaS startup, and can we reach profitability fast enough that it doesn’t become a balance sheet anchor?”
If the answer was yes, then Option B was the obvious choice. You’d be capturing a 25% margin pool that was currently leaking to external providers, while simultaneously solving the utilisation control problem that was inflating your insurance costs.
But to answer that question, they needed to understand why India’s healthcare infrastructure market was fundamentally different from the U.S. or Europe. They needed to understand why the dysfunction that made Indian healthcare expensive for patients made it structurally advantageous for integrated builders.
They needed to understand why India is different.
[IX] Why India, Why Now?
If the “Payvidor” model is so compelling, if Kaiser proved it decades ago and Optum is minting money with it now, you have to ask why the entire world isn’t just one giant integrated health system.
The standard answer is that it’s too hard. Incumbents can’t pivot without blowing up their existing revenue, and startups can’t raise the capital needed to build hospitals. It’s a “Capital and Patience” problem.
But India is currently a place where structural dysfunction has accidentally created a perfect laboratory for the Payvidor model. In India, the things that usually make life difficult for a business, extreme fragmentation and a total lack of legacy infrastructure, are actually your biggest strategic advantages.
Fragmentation is Leverage
In the United States, being a Payvidor means contending with consolidated incumbents. In many American cities, one or two hospital chains control 40% of the beds. If you’re an insurer, you’re their hostage, if they threaten to leave your network, your members riot. To control the system, you effectively have to buy the system, which is why UnitedHealth spent billions acquiring provider groups before Optum could work.
In India, fragmentation is your leverage.

The largest hospital chain in the country - Manipal - controls less than 0.5% of India’s beds. The top five chains combined don’t crack 5%. There are 15,000 different facilities competing for survival. If you are an integrated player with 100,000 members in Bangalore, you control roughly 5,000 hospitalisations a year. To a hospital sitting at 60% occupancy and sweating its debt service, those 5,000 patients are the difference between a good quarter and technical default.
In the US, the hospital owns you. In India, the person who aggregates the patients owns the hospital.
But as we saw earlier, aggregating demand alone isn’t enough. The patient has to trust you enough to go to the hospital you choose, which means you need to own the gatekeeping layer. Control the first doctor they see, and you control everything downstream.
This is done by controlling utilisation at the primary care level
In the West, “Primary Care” is a deeply entrenched legacy business. You have family doctors who have seen the same patients for thirty years in physical offices they own. They have autonomy, they have tenure, and they generally don’t want to become salaried employees of a tech startup.
India, by contrast, is a blank slate.
Before we go further, let’s define what we mean by “primary care” versus “secondary care,” because this distinction is critical to understanding why Even’s model works:
Primary Care is your first point of contact with the healthcare system. It’s the general physician you see for routine checkups, common illnesses (fever, cough, stomach issues), chronic disease management (diabetes, hypertension), preventive care (vaccinations, screenings), and referrals to specialists when needed. Primary care is low-complexity, high-volume medicine. It’s the doctor who knows your medical history and acts as the gatekeeper to the rest of the system.
Secondary Care is specialized care that requires hospital infrastructure but isn’t highly complex. This includes routine surgeries (appendectomy, gallbladder removal, hernia repair), childbirth, orthopedic procedures (fracture repairs, knee surgery), diagnostic procedures requiring sedation, and short hospital stays (2-3 days). Secondary care handles the bulk of healthcare volume - the predictable, routine procedures that people need regularly.
Tertiary Care is highly specialized, complex medical care. Think brain surgery, organ transplants, advanced cardiac interventions, cancer treatment with specialized equipment, Level 1 trauma centers. Tertiary care is low-volume but extremely capital-intensive, requiring expensive equipment, highly specialized physicians, and intensive care infrastructure.
For the emerging middle class in India, “Primary Care” as a consistent, longitudinal relationship with a family doctor barely exists. Healthcare is transactional and episodic. You see a different doctor each time you’re sick. There’s no accumulated medical history, no ongoing relationship, no physician who knows your family’s health patterns.
This lack of legacy infrastructure is a gift. It means you can leapfrog directly to telehealth-enabled primary care without disrupting entrenched physician relationships or practice ownership structures.
And because Indians are already culturally comfortable with remote care, thanks to over 300 million government-sponsored e-Sanjeevani teleconsultations proving the concept works, you can build a “gatekeeping layer” ten times faster than Kaiser ever could.

This is another major leapfrogging phenomenon for India in the 21st century.

India Builds Fast
Now we come to the advantage that really makes this model stand out in India.
In the United States, building a hospital is a multi-year, capital-intensive nightmare. You have to buy land, navigate permitting that can take years, comply with strict zoning and construction regulations, hire union labor, and build to handle every possible edge case. The result: hospitals take 3-5 years to go live and 2-3 years to reach breakeven.
In India, Even built their hospital in 7 months and reached breakeven in 6 months.

How is this possible?
The model is simple: you don’t buy land. You lease 50,000-80,000 square feet of commercial space in an urban area and re-build it as a hospital. Because you’re leasing rather than buying, you eliminate land acquisition costs and permitting delays. Because you’re retrofitting existing commercial real estate, construction is faster and cheaper than building from scratch.
More importantly, you don’t build for edge cases. You’re not constructing a tertiary care cathedral with oncology departments and robotic surgery suites. You’re building a secondary care facility focused on the high-volume, predictable procedures: routine surgeries, childbirth, orthopedic repairs, diagnostic procedures.
This is critical to understand: secondary care is where 70% of healthcare spending actually happens.
Nearly all insurance claims by volume sit in secondary care settings:
Maternity and childbirth
Routine surgeries (appendectomy, gallbladder, hernia)
Orthopedic procedures (fractures, joint issues)
Gynecological procedures
Diagnostic procedures requiring hospital setting
Short-stay hospitalizations (2-3 days)
Predictable events, not emergencies requiring a 2 AM rush into a tertiary care stack of ICUs and trauma teams, but planned procedures where the patient can choose where to go based on trust, convenience, and experience.
Here’s something interesting, and frankly mind-boggling.
India has a massive bed shortage. The country needs roughly 3 million additional hospital beds to meet WHO-recommended capacity. The conventional wisdom is that solving this would require $250 billion in capital investment, a staggering sum that seems impossible to raise.
But that $250 billion number is misleading. Here’s the actual math: roughly 80% of the bed shortage is for secondary care, while only 20% is for tertiary care. But because tertiary beds are so expensive to build, roughly ₹2.2 crores ($260,000) per bed for a fully equipped tertiary facility, they represent 80% of the capital requirement.
Secondary care beds, by contrast, cost about ₹20-25 lakhs ($24,000-30,000) per bed to build. One-tenth the cost.
This means you could solve 80% of India’s bed shortage, the part that handles the bulk of healthcare volume, for roughly $50-60 billion. Not $250 billion. $50-60 billion. The rest $200B is duly attributed to the remaining 20% of the total bed shortage, requiring tertiary care.
To put that in perspective: that’s less than what the top AI labs have collectively raised in the last three years. OpenAI, Anthropic, and a handful of AI startups have raised over $100 billion to build large language models. India could build enough hospital capacity to serve its entire population for half that amount.
The market is currently doing the opposite. Nearly all healthcare capital is flowing into tertiary care, the expensive, low-throughput part of the system that serves maybe 30% of the need. Meanwhile, secondary care, where the actual volume is, remains fragmented across thousands of low-quality clinics.
A tertiary bed costs ₹2.2 crores to build and takes years to reach breakeven. A secondary bed costs ₹20-25 lakhs and can reach profitability in months if you have patient flow (which Even does, through their insurance members and primary care gatekeeping).
The combination of aggregating fragmented hospitals through primary-care control and selectively building owned secondary care only where unit economics justify it, enables an integrated delivery model to scale ~10× faster than Kaiser’s fully owned-asset approach, at ~1/10th the capital intensity.
Even doesn’t have to buy the system (fragmentation means they can aggregate patient flow and control utilisation).
Even doesn’t have to disrupt entrenched primary care relationships (they can leapfrog to telehealth-first).
Even doesn’t have to build tertiary cathedrals (they build lean secondary care focused on the high-volume 70%).
For the cases that do require tertiary care, the brain surgeries, the complex cardiac interventions, the organ transplants, Even just contracts with existing tertiary hospitals. They don’t need to own that infrastructure because it’s only 20-30% of total healthcare spending. They own the 70% that matters: primary care (the gatekeeping layer) and secondary care (the volume layer)
The result is a model that captures most of the healthcare dollar at a fraction of the capital intensity. Even’s hospital cost $3.5 million and 7 months to build.
Given that the economics were this lopsided, the question for Even wasn’t whether they should own the concrete. It was why anyone would ever bother building anything else.
To that end, Even raised a $30 million Series B in October 2024, led by Khosla Ventures, with 8VC joining for the first time alongside returning investors Founders Fund and Lachy Groom. The mandate was straightforward: build a hospital in Bangalore.

[X] The Hospital (They Built in Seven Months)
Once you decide you need a hospital, the standard private equity move is to find someone who already has one and buy it. This is usually called “acquisition,” and in most industries, it is a way to skip the line.
Even looked at over sixty different hospitals in Bangalore and discovered that, in the Indian medical infrastructure, an acquisition is often just a very expensive way to inherit a criminal investigation. They found buildings purchased with unaccounted cash, fire safety certificates that were essentially works of fiction, and clinical documentation that wouldn’t survive a casual glance, let alone a regulatory audit.
More importantly, they realised that buying a hospital means inheriting its culture. If a doctor has spent a decade making 40% of his income from a revenue-share on cardiac stents, he is not going to be thrilled when you show up with a slide deck about “preventative care” and a fixed salary. You can retrofit a plumbing system, but you can’t easily retrofit a person who has a mortgage to pay and a commission-based mindset.
So, they decided to build. But they decided to build in a way that makes a traditional hospital investor feel like they are having a stroke. In August 2025, Even opened their first 70-bed hospital on Race Course Road in Bengaluru - on time, two percent within budget, and built in seven months inside a leased commercial space for $3.5 million.

The lease model was the key. By retrofitting existing commercial real estate rather than buying land and breaking ground, Even compressed the construction timeline from years to months. They designed the administrative processes from scratch, meaning they could do things that are obvious in hindsight but impossible in a legacy building (more on this later). And by hiring doctors into a salaried model from Day One, they avoided the toxic politics of compensation restructuring that kills most acquisition-led integration attempts.
If seventy percent of healthcare spending is in secondary care but ninety percent of capital flows to expensive tertiary facilities, the smartest thing you can do is build for the missing middle.

The real magic, however, was the math of demand visibility. A traditional hospital builds a massive facility and then spends years praying that patients show up, often while spending crores on marketing and sweating its debt.

Even built a facility that arrived with a pre-installed customer base - and the location wasn’t accidental. The member data they had accumulated across Bangalore told them exactly where their patients lived, which neighbourhoods had the highest density of members needing in-person care, and how far they were willing to travel.

Race Course Road in central Bangalore put the hospital within a 20-30 minute drive of the bulk of their member base in South and Central Bangalore. They didn’t have to hire “sales” doctors or worry about geographic catchment. They already knew the catchment. They just built where the data pointed.

When a procedure is recommended by an Even doctor and scheduled at an Even facility, roughly 50% of patients at the city level proceed to have it performed at the Even hospital, rising to approximately 75% for patients within a 5 kilometre radius. Even didn’t have to force members into a closed network, they could have chosen any of the partner hospitals empaneled across Bangalore. But it turns out that if you offer people a hospital that’s reasonably close to their home, with doctors who don’t treat them like a utilisation opportunity, they actually prefer being there. Experience matters more than brand recognition when you’re making healthcare decisions under stress

The hospital reached EBITDA breakeven in six months. The projected 37% IRR, which had been a hopeful number in their Series A deck, became real cash flow on the bank statement.
It turns out that if you engineer the incentives and workflow deliberately, you can build a hospital for about the price of a Series A round and have it profitable by the time a traditional builder has finished pouring the foundation for their second floor.

Is It Really Waiting If You Don’t Know Why?
Running a hospital revealed something important: a lot of what makes healthcare miserable isn’t the medicine, it’s the administrative plumbing.
Mayank noted that while India has plenty of people who know how to run hospitals, most of them are professionally committed to processes designed for hospital convenience, not patient experience.
Take the common experience of hospital discharge. The doctor clears you at 9 AM. You’re medically ready to leave. But then you sit in your room with your bags packed until 2 PM because the billing department is reconciling charges with the pharmacy, the administration is generating discharge summaries, and various departments are playing bureaucratic ping-pong while you wait.

You spend five hours in a state of packing-induced anxiety, dressed in street clothes, sitting on a hospital bed, feeling like a prisoner waiting for release papers.
Even’s solution is a lesson in what the behavioural economist Rory Sutherland would call a psychological moonshot. Sutherland’s core insight is that we habitually try to solve problems through physical or logistical means - build it faster, make it bigger, add more resources - when the cheaper and often more powerful solution is psychological. The experience of waiting isn’t just about time. It’s about what that time feels like. Change the feeling and you’ve solved the problem, often at a fraction of the cost of solving the logistics.
Applied to hospital discharge, the insight is almost embarrassingly simple: don’t tell the patient they’re discharged until the paperwork is already done.
The discharge process starts the moment the doctor decides you’re medically cleared, but the patient doesn’t know that. Behind the scenes, billing reconciles charges, pharmacy packages medications, administration generates summaries. When everything is ready, the staff walks in and says: “You’re all set. Here’s your discharge summary, here are your medications, you can leave now.”
The patient experiences a thirty-minute transition instead of a five-hour hostage situation. The work takes the same amount of time. The patient just spends that time feeling like a patient recovering in bed rather than a line item stuck in an administrative queue.
Though this sounds trivial. It’s not. In traditional hospitals, the patient waits for the system. In Even’s hospital, the system waits for the patient. That inversion, repeated across dozens of micro-processes, completely changes how people feel about the experience.

The Walk-In Problem
The biggest surprise wasn’t that Even members used the hospital. It was that non-members started showing up.
Within three months of opening, roughly 70% of the hospital’s patients were walk-ins, people who weren’t Even members but had heard through word-of-mouth that there was a new facility in the neighborhood that didn’t price-gouge, didn’t run unnecessary tests, and had doctors who actually explained things.
Now, 70% walk-in traffic might not sound like a needle-mover for a hospital business. But for an integrated business, it creates an accidental but powerful conversion funnel.
Here’s how it works:
A non-member comes in for a routine procedure, let’s say a minor orthopedic surgery or a diagnostic scope. They pay out-of-pocket or use their own insurer. The care is good, the facility is clean, and critically, there are no surprise bills, no “miscellaneous charges” appearing three weeks later, no estimate desk trying to upsell deluxe rooms.
At discharge, they have a brief conversation with the billing administrator: “By the way, did you know the hospital is run by Even Healthcare? We also offer health insurance. If you’d been a member, this procedure would have been fully covered under your annual premium.”
A certain percentage of these walk-ins convert. Not all of them, but enough. They’ve just experienced the product (integrated care delivery) and validated that it works in the highest-stakes moment possible (when they were actually sick).
For Even, this creates a beautiful dynamic: the hospital makes money on walk-ins through provider margin (standard hospital economics) and then converts a subset of those walk-ins into long-term insurance members (subscription revenue with high LTV).
Traditional hospitals can’t do this because they don’t sell insurance. Traditional insurers can’t do this because they don’t own hospitals. For Even, the hospital became the ultimate “Try Before You Buy” experience. It’s a physical manifestation of the brand’s promise.
The result is a business that captures provider margin on everyone who walks through the door (member or not) and captures insurance margin on the subset that converts to membership. Even built a system where being fair to the patient, no surprise bills, no unnecessary tests, transparent pricing, is actually the most efficient way to scale the balance sheet.

[XI] The Even Lesson
There’s a broader pattern here that applies far beyond healthcare, and it’s worth calling out explicitly because it’s one of the most powerful but under-appreciated business model innovations.
Most businesses separate “making the thing” from “selling the thing.” This creates an inherent tension: the incentive to make the best product is in tension with the incentive to sell the most product. Sales teams push features customers don’t need. Product teams build things the market doesn’t want. The feedback loop is broken because the people making decisions about the product never see the full customer journey.
Even collapsed that separation. They don’t “make healthcare” and then “sell insurance.” They do both, and the doing of one makes the other better.
Essentially the most durable businesses are those where owning one layer of the stack automatically makes every other layer more valuable - where the act of improving the product is indistinguishable from the act of defending the business.
This is a generalisable pattern, and it shows up in every category where integration wins:
Tesla doesn’t just make electric cars, they own the charging network and the software updates. The car becomes better over time, which makes the brand stronger, which increases willingness to pay, which funds more charging stations, which makes the car more useful. The loop closes.
Apple doesn’t just make phones, they control the App Store and the services ecosystem. The hardware and software make each other better. A great iPhone app makes the iPhone more valuable. A large iPhone install base makes app development more lucrative. The loop closes.
Amazon doesn’t just sell products, they own the logistics network and increasingly, the product creation (private label). Fast shipping makes the marketplace better. Marketplace data tells them what products to build. The loop closes.
The pattern: own enough of the value chain that improving the customer experience directly improves your economics, not just your NPS score
In fragmented industries, “delighting the customer” is a cost center. You spend money on better service, and you hope it leads to retention and word-of-mouth, but the connection is indirect and hard to measure.
When you own the full stack, doing the right thing for the customer and doing the right thing for the business become the same thing. That’s not because you’re virtuous. It’s because you’ve aligned the incentives such that the most profitable action is also the fairest one.
This is the hardest business model to build (you need more capital, more operational complexity, more expertise across domains), but it’s also the most defensible once built. Because competitors can copy your product, they can copy your pricing, they can copy your marketing, but they can’t copy the structural alignment that comes from owning the whole loop.
Even didn’t set out to teach a lesson about vertical integration. They just wanted to fix a broken healthcare system. But in the process, they’ve demonstrated something that applies to almost every industry with misaligned incentives: the best way to win is to own enough of the value chain that “doing right by the customer” stops being a trade-off and becomes the strategy.

Now, How Does Even Actually Make Money?
By September 2024, the Even model had evolved from a mission-driven experiment into a four-layer vertical funnel designed to capture every available rupee of margin while systematically de-risking the balance sheet.
The system works through a series of filters designed to catch health issues before they escalate into expensive hospitalizations:
Layer 1: Telehealth Primary Care (Up to 85% of issues resolved here)
In a traditional insurance model, the company gives you a card and then hides, hoping you never use it. At Even, the goal is for you to call them immediately. Why? Because the marginal cost for Even to have its salaried doctor tell you over the phone that your cough is just a cough is zero.
If you hadn’t made that call, you might have panicked and gone to an external Emergency Room, which would have resulted in a ₹5,000 bill for “observation” and a series of defensive tests. By spending ₹300 on a phone call, Even has probably avoided a ₹5,000 claim. That is a magnificent arbitrage of physician time against hospital overhead.
Layer 2: Owned Clinics (10% of issues need in-person care)
If the phone call doesn’t work, you go to the clinic. This is where Even captures the “Hands-On” margin. In India, if you send a patient to an external lab for a blood test, you are paying for that lab’s profit margin. If Even owns the lab, they keep the change (and pass it on the patient). But more importantly, the clinic acts as a second filter. It handles the minor procedures and the chronic monitoring that, if ignored, eventually turn into the kind of catastrophic events that require an ICU bed.
Layer 3: Owned Secondary Care Hospital (3.5% of episodes of care, 70% of inpatient needs handled here)
This is where Even internalizes the “Routine 70%.” Most surgery is not a medical mystery. Having a baby or getting your gallbladder removed are high-volume, predictable, scheduled events.
By owning the operating room, Even captures the 25% “Provider EBITDA” that we talked about earlier. In any other insurance model, that 25% is a “Medical Loss.” In Even’s model, that 25% is “Internal Revenue.” They have essentially turned their biggest liability, the hospital bill, into their most profitable asset.
Layer 4: External Tertiary Care (20-30% of total spend goes here)
For the small fraction of cases that require genuinely complex intervention - brain surgery, organ transplants, advanced oncology - Even coordinates care with external specialist hospitals and the partner carrier covers the claim.
Even doesn’t own ₹15 crore robotic surgery suites, since capital-intensive equipment tends to work best in models built around consistently high utilisation. The black swans get outsourced. Even manages the care pathway to make sure the specialist isn’t running a utilisation play and lets someone else worry about the mortgage on the equipment.
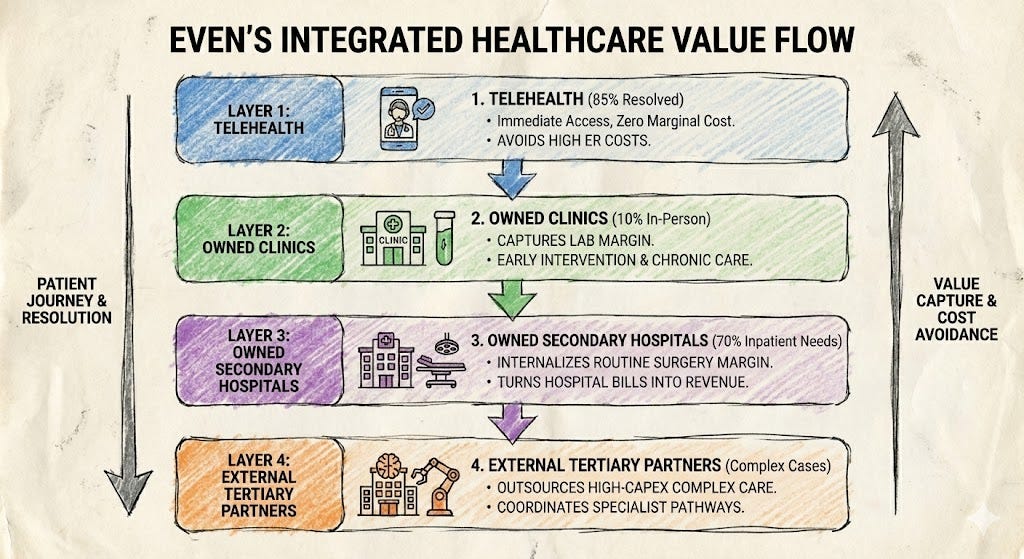
The Internalisation Math
Here’s the critical insight: at each layer, the integrated model captures margin that would normally go to external providers.
By September 2024, Even was internalising approximately 70-80% of total healthcare spending across their member base. That means 70-80% of the money that would normally flow out to external hospitals, labs, and specialists was instead staying within the system.
The remaining 20-30% going to external tertiary specialists still generated insurance-related fees on the total book, while the partner carrier bears the underwriting risk. But the care delivery and provider margin capture works the same way regardless of operating model.
This is where economics gets beautiful. Even is capturing both profit pools that normally exist in separate companies:
Provider Margin (on the 70-80% internalized):
Clinics run at 30-35% EBITDA margin
Hospital runs at 25-30% EBITDA margin
Diagnostics run at 40-50% EBITDA margin (high-margin business once equipment is paid off)
Insurance Margin (on the total book):
Collect premiums from all members
Pay claims (mix of internal cost + external tertiary care)
Keep the spread
Insurance EBITDA typically 3-7% of gross written premiums
The blended result: Even’s combined EBITDA margin runs 23-26% depending on internalization rate and case mix.
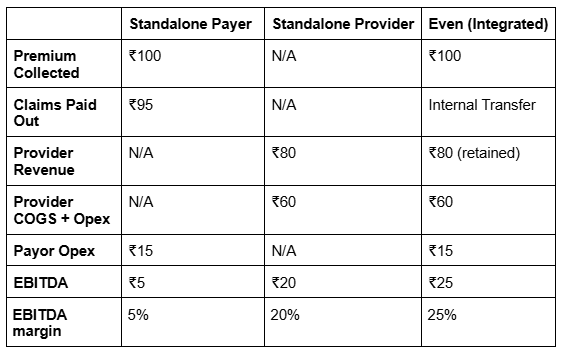
A standalone hospital captures provider margin on whoever walks through the door - 20-25% EBITDA, a good business, but one that lives and dies by volume and has no insurance upside. A standalone insurer collects premiums and pays claims, generating 2-5% EBITDA on a model that has no control over the utilization it’s paying for. Both are trapped in the adversarial relationship we’ve spent thirty thousand words describing.
Even captures both margin pools simultaneously. The insurance business generates commission income on the total member book. The provider business generates 20-25% EBITDA on the care it delivers internally. The blended result - 23-26% EBITDA - isn’t remarkable because the individual margins are high. It’s remarkable because a standalone insurer would record Even’s provider margin as a claims cost. Even records it as revenue. The same rupee that leaves one pocket enters the other.
The Claims Ratio Advantage
The clearest evidence of how this plays out sits in the claims ratios of Even’s partner carrier’s book. Even’s B2C portfolio runs at roughly 40% claims ratio, against an industry average of 55% for standalone insurers. The B2B side tells the same story - Even runs corporate portfolios at roughly 85% claims ratio, against an industry average of 95-105%, a spread significant enough that traditional insurers often lose money on group policies entirely.
The mechanism behind both numbers is the same: when care flows through owned delivery rather than through external hospitals with every incentive to maximise the bill, the cost structure changes fundamentally.
It’s worth being precise about how Even actually captures this, because it’s a common source of confusion. Even’s insurance income is a fee business, not an underwriting business. The spread between premiums and claims belongs to the partner carrier’s P&L, not Even’s. When Even’s book runs at a 40% claims ratio against an industry average of 55%, the partner carrier is the one booking that underwriting profit.
What Even captures instead is a contractual share of the savings they generate. Even charges the partner carrier at cost for actual procedure delivery, and then earns 80% of the savings relative to what the same care would have cost at an external hospital. If Even delivers an appendectomy for ₹60,000 in marginal costs against an external market rate of ₹1,20,000, they earn 80% of the ₹60,000 delta on top of cost recovery. The incentive to keep delivery costs low is therefore direct and contractual, the cheaper Even can deliver care, the larger the savings pool they’re splitting with the carrier.
This is what makes the claims ratio a genuine proxy for Even’s own economics. A deteriorating claims ratio doesn’t just threaten the partner carrier’s underwriting profit. It directly compresses Even’s margin.
There’s a compounding effect that operates on the consumer side too. A structurally lower cost base doesn’t just improve Even’s margin, it allows them to price the insurance product itself more competitively than standalone carriers can. In a market as price-elastic as retail health insurance, where premium sensitivity is the single biggest barrier to adoption, this matters enormously. The integrated model doesn’t just make Even more profitable than a standalone insurer. It makes them cheaper than one too. In a market where customers struggle to distinguish between policies, price is the decision variable. Even’s cost structure lets them win on that dimension without sacrificing margin to do it.
The Retention Flywheel
The most important metric, however, isn’t margin. It’s retention.
In traditional insurance, healthy people leave (they’re subsidizing sick people and they know it) while sick people stay (pre-existing condition clauses trap them). The pool gets sicker over time. Premiums rise. More healthy people leave. Deaths spiral.
Even has flipped this dynamic entirely.
Members actively engage with the product. The average Even member has 8-10 touchpoints with the healthcare system annually (including telehealth calls, clinic visits, diagnostic tests, and routine check-ups), with a minimum of 4 proactively initiated by Even through scheduled outreach. The industry average is 1-2 touchpoints per year, typically a single acute illness episode.
That gap between a healthcare relationship and a healthcare transaction, is where Even’s business actually lives. When you use something regularly and it works well, you don’t leave.
By Quarter 5 (15 months after joining), Even’s retention rate is near 100%. Not because members are contractually trapped, Even doesn’t exclude pre-existing conditions aggressively. The retention exists because the product works in the way products rarely work in healthcare: consistently, over time, in ways that become harder to replicate the longer the relationship runs. Customer acquisition cost that would amortise over two years at industry-standard churn rates amortises over much longer periods. The math of the business changes entirely.
This is the ultimate validation that the model works. Members stay because:
They’re using the clinics regularly (proximity, convenience)
They’ve built relationships with their doctors (switching cost)
They’ve had good experiences when they needed care (trust)
The insurance actually pays claims without fighting them (reliability)
High retention means:
Customer acquisition cost amortizes over 5-7 years instead of 2-3 years
Members get healthier over time (continuous care management)
Adverse selection is avoided (balanced pool of healthy and sick members)
Lifetime value of a member is 3-4x higher than traditional insurance
Mayank summarizes the core business model: “We don’t do healthcare to make money. We do healthcare to make insurance cheaper.”
By owning the care delivery, Even has:
Solved the “Headache MRI” problem (no over-treatment)
Captured the diagnostic profit (own the labs)
Filled their own hospital beds without spending on marketing (organic routing)
Built a business with the revenue visibility of insurance and the margins of hospitals
Even has built a system that is structurally more efficient than either standalone player could ever be. The unit economics prove it. The retention proves it. The claims ratios prove it.
But unit economics alone doesn’t build a durable business. A 25% margin in a $100 billion market eventually attracts attention.

[XII] Moats
Would Your Board Let You Kill Your Most Profitable Business?
If you are a multi-billion-dollar incumbent in the Indian healthcare market, you have spent the last two years watching Even Healthcare prove that the payvidor model works. You have seen the spreadsheets showing 25% EBITDA margins and 40% claims ratios. You have read the pitch decks. And you have probably asked yourself: “Why don’t I just do that? I have the hospitals, I have the doctors, and I have more money than God. I should be able to crush these people on the weekend.”
The answer is that you can’t, because you are currently trapped in a very successful, very profitable cage of your own making.
From the perspective of a would-be disruptor, Narayana Health is not some cautionary tale about a bad strategy. But it is an illuminating tale about what happens when a genuinely good strategy collides with a genuinely good existing business. Narayana has built one of the most admired hospital chains in the world - the high-volume, low-cost masters of cardiac surgery. When Narayana launched Narayana One Health in 2024, it was a logical extension of everything they’d built.
Before we talk about what Narayana couldn’t do, it’s worth pausing on what it did. Dr. Devi Shetty - cardiac surgeon, son of a spice trader from coastal Karnataka, man who once operated on Mother Teresa - built something that most people in global healthcare still consider impossible.
In the 1990s, when the received wisdom was that quality cardiac surgery required either a wealthy patient or a Western zip code, Shetty looked at the economics differently. He asked what cardiac surgery would cost if you did enough of it - if you applied to the operating room the same logic that Henry Ford applied to the assembly line.
The answer, it turned out, was a fraction of what anyone had been charging. Narayana’s Mazumdar Shaw Medical Center in Bangalore performs more open-heart surgeries annually than almost any facility in the world, at prices that make American hospital administrators physically uncomfortable. Shetty proved that high volume and high quality are not opposites in medicine, that the surgeon who does 600 procedures a year is almost certainly better than the one who does 60, and can charge less for the privilege.
If Even is trying to answer the question “what does healthcare look like when the incentives are right,” Devi Shetty answered an earlier version of the same question thirty years ago, with a scalpel and a spreadsheet. The challenge of the Narayana One Health journey is not that Shetty misunderstood integration, if anything, he understood it earlier than most. It’s that he built something so successful, on such specific economics, that layering insurance on top means asking a finely tuned machine to run a different program while still doing what it was built to do. That’s not failure. That’s the hardest kind of problem: the one created entirely by your own prior success.
When Narayana launched Narayana One Health in 2024, it looked like that problem was about to be solved. On paper, it was a slam dunk. They had 49 hospitals, 7,000 beds, and decades of operational excellence. Eighteen months later, Narayana had sold around 75,000 policies. For context, the Indian market sells about 26 million a year.
To understand why, you have to understand a few traps that caught Narayana, and why those same traps would catch any incumbent trying to replicate Even’s model.
Narayana’s hospitals run on a specific financial model: high volume, moderate complexity, aggressive utilisation. Their cardiac programs are profitable because they do a lot of surgeries. Their EBITDA depends on keeping operating rooms at 70-80% utilisation.
When Narayana launched NOH, they immediately faced a contradiction:
As a hospital, they make money when patients need surgery
As an insurer, they make money when patients don’t need surgery
Every elective procedure that NOH prevents is revenue that Narayana Health loses. Every unnecessary test that an NOH care coordinator questions is margin that the hospital was counting on.
In theory, the solution is simple: measure success at the holding company level (consolidated EBITDA), not the subsidiary level. Optimize for total profit, not hospital revenue.
In practice, this requires blowing up the internal incentive structure of a 30-year-old hospital business.
The Narayana hospital CEOs are measured on bed occupancy, revenue per bed, and EBITDA margin. They have debt covenants tied to these metrics. Their bonuses depend on hitting utilisation targets.
If NOH starts routing fewer patients to Narayana hospitals, or if they start pressuring doctors to be more conservative with procedures, the hospital CEOs revolt. If the CFO sees cardiac revenue dropping because NOH is managing chronic patients out of the operating room, the Board asks very pointed questions about why they’re cannibalising a profitable business to subsidise an unproven insurance experiment.

Even solved this by not having a legacy business to cannibalise. They started as an insurer and built the hospitals specifically to serve the insurance model. The incentives were aligned from Day One because there was no prior structure to fight against. There was no hospital CEO whose bonus depended on keeping beds full. There were no doctors on commission wondering why the new insurance product was reducing their surgical volume.
Narayana’s top surgeons work on a revenue-share model. A senior cardiac surgeon at Narayana might make ₹1.2 crores annually, with 40-50% of that tied to surgical volume.
When NOH launched, they needed these same doctors to act as “gatekeepers” who would triage patients conservatively, manage chronic conditions, and avoid unnecessary procedures. They needed them to act like salaried Even doctors.
But Narayana couldn’t just convert them to salary. These doctors had mortgages, lifestyles, and expectations built on commission income. If Narayana tried to restructure their comp, the doctors would leave for Apollo or Fortis, taking their patient relationships with them.
The compromise: NOH members still got routed to Narayana hospitals, but the doctors operated under the same revenue-share model. The only difference was that NOH (instead of the patient or a third-party insurer) was paying the bill.
This doesn’t solve the utilisation problem. It just moves who writes the check. The doctor still has an incentive to maximise procedures, and the hospital still has an incentive to fill beds. NOH didn’t internalise the adversarial relationship, they just made themselves both sides of the fight.
Even, by contrast, hired doctors into a salaried model from scratch. They selected people who were tired of the commission treadmill. The doctors who joined Even were making a specific trade: give up commission-based income volatility in exchange for predictable salary, equity upside through ESOPs, and the ability to practice evidence-based medicine without prescription targets.
After two years, these doctors are culturally locked in. They’ve experienced what it’s like to practice medicine without having to justify every decision to the unit head. If a competitor tries to poach them with a higher salary, they’re not just competing on comp. They’re asking the doctor to go back to a system they already left.
There is a third gap that doesn’t show up in any org chart. Even has three years of closed-loop data that no standalone player can see. An insurer watching a member’s file sees a claim for a pre-diabetes consultation. A hospital treating the same member sees an HbA1c result. Even sees the whole arc: the screening that caught it, the intervention that followed, the quarterly monitoring that kept it from progressing, the hospitalization that never happened. That invisible data point, the outcome that didn’t occur, is the most valuable piece of information in the file, and it only exists if you own both the insurance and the care.
A competitor who opens today and does everything right will have good outcomes. They won’t have Even’s outcomes. Not yet. In chronic disease management, where the relevant timescale is decades, “not yet” is a meaningful gap.
Another major reason Even’s model works is because they control the first touch. When a member feels sick, they call Even’s telehealth line. The Even doctor decides whether it’s a primary care issue (handle in-clinic), a secondary care issue (route to Even hospital), or a tertiary issue (send to external specialist).

Narayana doesn’t do primary care, the way Even does. They have hospitals built for secondary and tertiary care. They have only recently started building out neighbourhood clinics. Moreover, they don’t have salaried GPs doing telehealth triage.
When an NOH member gets sick, they don’t call a “Narayana primary care doctor.” They either:
Go directly to a Narayana hospital (expensive, over-treatment risk)
See an external GP (Narayana loses control of the care pathway)
Call a third-party telemedicine service (no integration with Narayana’s systems)
Without owning primary care, Narayana can’t control utilisation. They can’t catch the diabetic before the amputation. They can’t manage the hypertensive before the stroke. They’re still operating as a reactive “repair shop,” not a proactive health system.
Building primary care from scratch means:
Leasing clinic space in 10+ neighbourhoods across each city
Hiring 100+ salaried GPs who don’t exist in the current market
Building a telehealth platform and training doctors to use it
Waiting 12-24 months for geographic “catchment” to build
This is a ₹100-200 crore, multi-year project that competes with the core hospital business for capital allocation. The hospital division needs that capital to expand bed capacity and service debt. The insurance division is a subscale experiment that won’t generate meaningful revenue for years.
Which business gets the capital? The one that pays the bills today, or the one that might pay the bills in 2027?
Meanwhile, Even already has the clinics, the doctors, and the members trust. They’re profitable at the clinic level and use that cash flow to fund hospital expansion. The capital incentives are aligned.
Here’s a question that Narayana didn’t anticipate: Why would someone buy insurance from a hospital chain?
When you think of Narayana, you think “cardiac surgery” and “hospital beds.” You don’t think of “comprehensive health management” or “preventative care.” The brand is built around intervention, not avoidance.
If you’re a healthy 30-year-old, do you want to buy insurance from a company whose business model depends on you eventually needing surgery? The psychology is backwards. There’s an implicit distrust: “Are they going to keep me healthy, or are they going to find reasons to admit me to one of their hospitals?”
Shetty learned this the hard way, admitting: “We severely underestimated how much insurance is about selling.”
If Narayana, with Viren Shetty’s strategic clarity and operational expertise, struggled with this, why would Apollo or Max or Fortis try?
The answer: they are trying, but through acquisition rather than organic build.
In 2023, Manipal Hospitals (backed by TPG) started exploring partnerships with digital health insurers. Apollo has been in talks with several insurtech startups about co-branded products. The strategy is to buy the insurance capability rather than build it.
But acquisition doesn’t solve the incentive problem. If Apollo buys an insurtech and tries to route members to Apollo hospitals, they inherit the exact same conflict that’s strangling Narayana’s economics. The hospital still wants high utilization, the insurer still wants low claims. Changing the corporate structure doesn’t change the math.
The only way acquisition works is if the acquirer is willing to:
Blow up the hospital’s revenue model
Convert all doctors to salary (destroying retention)
Build a primary care network from scratch
Accept 2-3 years of depressed EBITDA while the culture resets
Convince the board that cannibalizing a profitable hospital business to build an unproven insurance business is a good use of shareholder capital
No public company CEO is going to do this voluntarily. The board would fire them before the first earnings call.

What about the other side? Can Star Health or ICICI Lombard just build hospitals and become Payvidors from the insurance direction?
In theory, yes. In practice, they have a different problem: they don’t know how to run hospitals.
Insurers are financial companies. They hire actuaries, underwriters, and claims processors. They don’t hire orthopedic surgeons, hospital administrators, or people who know how to negotiate with medical equipment vendors. They don’t know how to manage nurse retention, maintain ICU sterility protocols, or handle biomedical waste disposal.
If Star Health tried to build a 70-bed hospital, they would either:
Hire an external hospital management company (which defeats the purpose of vertical integration, you’re just paying a middleman with a different contract structure)
Promote internal people with no hospital experience (and watch the project fail spectacularly when they can’t handle the operational complexity)
Acquire a hospital chain (see the Narayana case study for why this doesn’t work, you inherit the culture and the incentive conflicts)
Moreover, insurers are terrified of taking on provider risk. Their entire business model is built on being the “payer” who can walk away if a hospital gets too expensive. Owning the hospital means you can’t walk away. You’re stuck with the capex, the fixed costs, the regulatory liability, and the operational headaches.
The insurer’s competitive advantage is negotiating with hospitals, not being one. Building hospitals would mean abandoning their core competency and entering a business where they have no muscle memory.
There’s a reason UnitedHealth spent 15 years and tens of billions of dollars building Optum: it’s a fundamentally different business that requires different talent, different culture, and different capital allocation. It’s not something you can spin up in a board offsite with a consulting deck.
The incumbents know the Payvidor model is better. They’ve seen the Kaiser numbers, they’ve watched Optum’s margins, and they’ve read Even’s pitch deck (either directly or through the VC gossip network).
They just can’t execute it without destroying the business that pays their salary today.
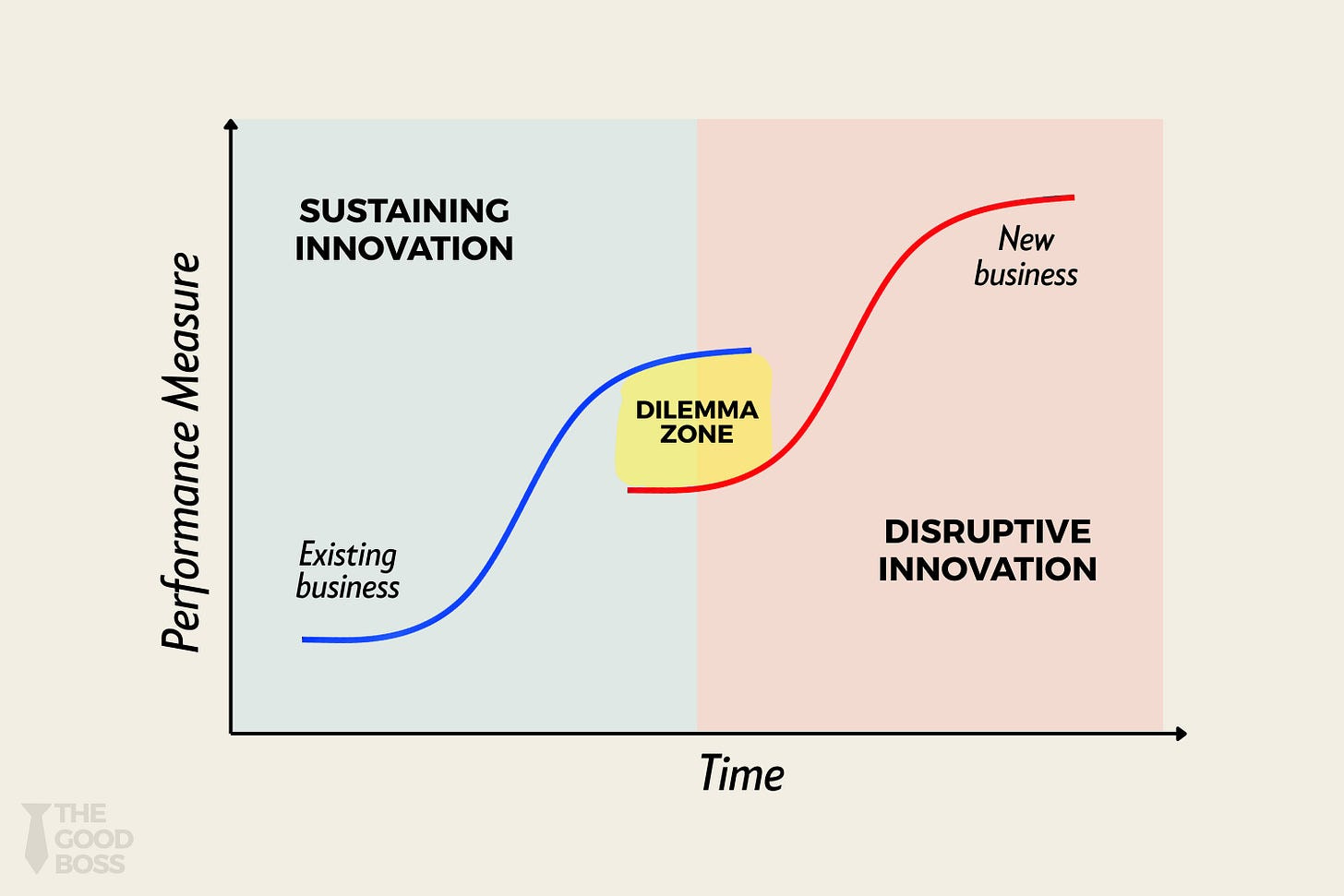
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
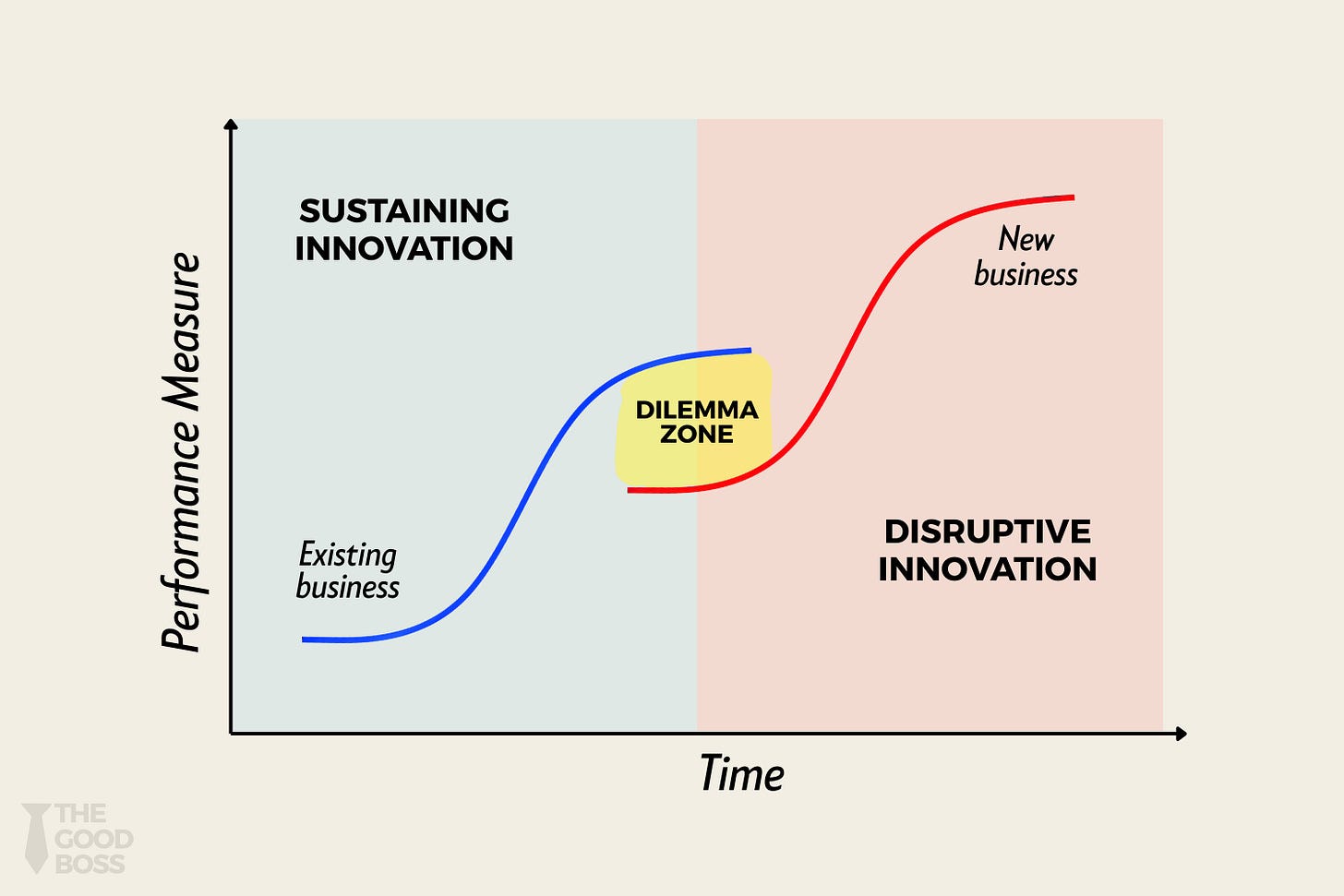{kind=link}
This is Clayton Christensen’s Innovator’s Dilemma in its purest form:
Hospital chains can’t become Payvidors without cannibalising hospital revenue
Insurance companies can’t become Payvidors without building hospital expertise
Both are trapped by quarterly earnings pressure and boards that won’t tolerate 3-year transformation timelines
In contrast, every month Even operates, they:
Add members (growing the data moat)
Train doctors in the salaried model (growing the talent moat)
Build facilities (growing the infrastructure moat)
Refine clinical workflows (growing the operational moat)
Collect longitudinal health data (growing the underwriting moat)
By the time Apollo or Star Health figures out how to navigate the internal politics of vertical integration, Even will have 500,000 members, 50 clinics, and 5 hospitals. The gap won’t be closeable with tactics. It will require strategy, capital, time, and a willingness to blow up a profitable business, four things that public company CEOs don’t have when the quarterly earnings call is in six weeks and activist investors are circling.
Even isn’t winning because they’re smarter than Viren Shetty (they’re not). They’re not winning because they have better technology than Apollo (they probably don’t). They’re not winning because they have more capital than Star Health (they definitely don’t).
They’re winning because they’re structurally free to build the right thing, while the incumbents are structurally trapped trying to build the wrong thing slightly better.
Narayana Health learned that you can’t integrate two businesses with opposing incentives by putting them on the same balance sheet. You have to build the integration into the DNA of the company from Day One.
Even did exactly that. And now the incumbents are learning that watching someone else do it right is much easier than doing it yourself.
The strangest part of what Even has built is that none of it was designed as competitive strategy. The salaried doctors weren’t hired to create switching costs; they were hired because commission-based medicine was showing up in the claims data. The clinics weren’t built to create density; they were built because 30% of care requires a physical examination and routing those patients externally meant losing control of the quality. The data accumulated because being integrated meant being the only entity in the system that could see the whole patient.
The defences emerged from trying to solve the problem correctly. Which is the most durable kind because it means the moat and the mission are the same thing. Even can’t be undermined by a competitor who simply decides to be fairer to patients, because being fairer to patients is exactly how Even built its advantage in the first place.

[XIII]: The Endgame
What If the Insurer Wanted You to Show Up for Every Sneeze?
If you follow the “Payvidor” logic to its jagged edge, you arrive at a conclusion so counter-intuitive it sounds like financial heresy.
In a traditional fragmented system, friction is a feature. Copays, deductibles, reimbursement paperwork - none of this exists to be cruel. It exists because the insurer has no control over what happens once you walk through a hospital door. Every visit is a potential utilisation event they can’t manage. So they install friction at the entry point to make you ask: “Is this chest pain really worth ₹1,000 and three hours of paperwork?” The bet is statistical, most deterred visits are frivolous, so the savings outweigh the risk of a missed signal.
But when you integrate the full stack, when the person paying for the care and the person delivering the care are the same entity, the physics of the system flip.
Suddenly, friction becomes the most expensive thing on the balance sheet.
If Even owns the clinic and the doctor’s time is already a fixed salary cost, the marginal cost of one more consultation is essentially zero. But the marginal risk of a member skipping that consultation is massive. In the old world, friction reduces utilisation on average, which helps the insurer’s quarterly P&L, even though specific missed signals will compound into catastrophic costs. The bet is statistical: most deterred visits are frivolous, so the savings outweigh the risk. In Even’s world, that bet disappears. Every missed signal is a deferred catastrophe they’ll have to pay for themselves.
Let’s say a member has a persistent, nagging cough. In a friction-heavy system, they wait. They don’t want to pay the ₹500 OPD fee. They don’t want to deal with the reimbursement. Three weeks later, that cough is a full-blown pneumonia hospitalisation that costs the insurer ₹50,000.
Now, in an integrated system, the same member has the same cough. Because there is zero friction, no copay, no “estimate desk,” just a seamless “walk in and see your doctor”, they show up on Day 2. The doctor spends ten minutes, realizes it’s a minor infection, and gives them a ₹200 strip of antibiotics.
From a structural perspective, Even would rather have you show up for ten “false alarms” than miss one “signal.” Ten false alarms cost them almost nothing in incremental overhead. One missed signal costs them a week’s worth of ICU bed-days.
This leads to a radical emergent possibility: The Zero-Marginal-Cost Patient.
If the goal is to maximise the “Prevention Profit,” the logical endpoint isn’t just “better insurance.” It is the total removal of the “transaction” at the point of care. If you make primary care, diagnostics, and basic medicines “free”, subsidised entirely by the premium and the captured provider margin, you aren’t being charitable. You are being ruthlessly efficient.
Now, to be clear, traditional insurers have figured this out too. That’s why you see global players offering Fitbits, gym memberships, and wellness credits. Prevention isn’t Even’s secret. It’s Econ 101.
But here’s the structural distinction: those programs are add-ons, not system redesigns.
A traditional insurer offering a free annual check-up still routes you through a third-party diagnostic lab and bills themselves ₹3,000 for a lipid panel. Even routes you through their own clinic, where the marginal cost is a ₹200 reagent kit and ten minutes of a salaried doctor’s time. The insurer subsidises prevention. Even internalises it.
The insurer gives you a Fitbit and hopes you use it. Even removes every behavioural barrier between “I feel weird” and “I’m sitting in front of a doctor.” The former is an incentive. The latter is a system.
This is why the unit economics diverge so violently. A traditional insurer can pay you to want to be healthy. But they can’t eliminate the friction that prevents you from acting on that want. You still face copays. Reimbursement forms. Network restrictions. Three-week wait times for specialist appointments. The prevention benefit is real, but the execution layer is still fragmented, expensive, and designed to ration care.
Even’s advantage isn’t discovering that prevention pays off. It’s that they can deliver prevention at zero marginal cost and zero friction, because they already own the infrastructure.
You are effectively paying your members in “convenience” to act as an early-warning sensor for your own insurance risk.

{kind=link}
By de-risking the “check-up,” you de-risk the “balance sheet.” You turn your customer base into a massive, distributed diagnostic network. Instead of rationing care through friction, you encourage care through abundance, knowing that a ₹1,000 “over-utilization” today is the only way to prevent a ₹10 lakh loss tomorrow.
This is the ultimate inversion. In the traditional model, the hospital prays you’re sick and the insurer prays you stay home. In the integrated model, both pray you come in early.
Whether this manifests as a specific product feature or simply a “frictionless” user experience, it represents the final stage of the Payvidor evolution. Once you own the full stack, the price of “appropriate care” tends toward zero, because that is the only price that perfectly aligns the patient’s health with the company’s survival.
In the long run, the most profitable way to run a healthcare system might be to stop charging for it.
The Risks Nobody Wants to Say Out Loud
If you’ve been reading carefully, you might have noticed something uncomfortable: we’ve spent 30,000 words explaining why fee-for-service creates terrible incentives (do more procedures = make more money), and now we’re celebrating a model that simply flips the incentive in the opposite direction (do fewer procedures = make more money).
The problem is that the opposite of a bad incentive isn’t necessarily a good one. It’s often just a different kind of bad.
When you own both the insurance risk and the care delivery, prevention becomes profitable. That’s the whole thesis. But “prevention becomes profitable” can manifest in two very different ways:
Version A (the idealized model): Your diabetic patient gets excellent preventive care, regular monitoring, medication management, and lifestyle coaching. You spend ₹5,000 annually keeping them healthy, which saves you ₹50,000 in hospitalization costs down the line.
Version B (the dark mirror): Your diabetic patient needs a minor surgical procedure that would cost ₹25,000 and take two weeks to schedule. Your salaried doctor, who is now measured on “cost per member” rather than “revenue per patient,” decides to manage it conservatively. Three months of medication and monitoring instead. The patient’s condition worsens. By the time surgery becomes unavoidable, it’s now an emergency procedure costing ₹1,50,000.
Both versions are “prevention” on paper. Both are rational responses to the incentive structure. The difference is that Version A makes the patient healthier and the company more profitable. Version B makes the patient sicker and the company bankrupt.
This is the Payvidor’s original sin: you’ve solved the over-treatment problem by creating the under-treatment problem.
The classic case study comes from the early days of HMOs (Health Maintenance Organisations) in the United States during the 1980s and 90s. HMOs were an earlier iteration of the integrated model: insurers who employed doctors and made money by keeping costs down. The incentive structure worked exactly as designed, costs went down. But so did patient satisfaction, clinical outcomes in certain categories, and trust in the system.
Patients began complaining about “gatekeeping” doctors who wouldn’t refer them to specialists. Physicians complained about being pressured to see more patients in less time and to avoid expensive treatments. By the late 1990s, “HMO” had become a term of abuse, shorthand for a system that prioritised profit over care.

Even mitigates this by measuring doctors on their health outcomes like re-admission rates over financial outcomes that would lead to more perverse incentives for the doctor to effectively deny care for their patients.
Here’s where it gets philosophically interesting.
Even’s model works beautifully if you assume members stay with the system for decades. If you’re managing someone’s health from age 30 to 70, the math of prevention is unambiguous. You invest ₹50,000 in cardiovascular health at age 45, and you save ₹5 lakhs in cardiac interventions at age 60. The ROI is extraordinary, as long as the member is still your member at age 60.
But what if they leave at age 50?
Now you’ve spent ₹50,000 on prevention, and your competitor gets to harvest the savings. You’ve effectively subsidized someone else’s balance sheet. The economically rational response, if you expect members to churn, is to under-invest in long-term prevention and focus on short-term cost control.
This is the time horizon problem. Insurance companies typically model a 3-5 year retention curve. But the health interventions that actually matter, diabetes management, hypertension control, cancer screening, these pay off over 10-20 years. If your financial model and your clinical model are operating on different time horizons, you get systematic under-investment in the things that actually keep people healthy.
Even’s current retention rate of near-100% by Quarter 5 looks great. But they’re still a young company with a relatively healthy member base. What happens when they have 500,000 members, including the sick, the old, and the price-sensitive?
The perverse outcome: the company that does prevention right might lose members to the company that does prevention wrong, because the benefits of good prevention are invisible (you don’t notice the heart attack you didn’t have), while the costs are immediate (higher premiums).
Mayank has thought about this problem, and his answer is both clever and slightly unsettling: “The only way to truly align incentives over a lifetime is to also sell life insurance.”
Here’s the logic: If Even is just your health insurer, they want to keep you healthy enough to not file expensive claims, but they don’t particularly care if you live to 90 or 70. The financial incentive stops at “keep them out of the hospital.”
But if Even is also your life insurer, they’ve just sold you a ₹50 lakh policy that pays out when you die, suddenly they have a massive financial incentive to keep you alive as long as possible. The longer you live, the longer they collect premiums without paying the death benefit. Prevention isn’t just about avoiding hospitalization costs anymore; it’s about delaying mortality itself.
This is technically called “longevity risk transfer,” and it’s the most aligned incentive structure you can create. The company literally makes more money the longer you live.
But it also creates a slightly dystopian flavor. Your healthcare company is now financially motivated to keep you alive, even if the marginal quality of life is low. Do they push aggressive interventions on a 75-year-old cancer patient because the alternative is a ₹50 lakh payout? Do they over-invest in longevity at the expense of quality of life?

But some argue this is overthinking it. The current system has zero incentive to keep you alive once you’re unprofitable as a patient. At least this model is trying to align financial incentives with clinical outcomes. Is it perfect? No. Is it better than a system that makes money by doing unnecessary surgeries on healthy people? Absolutely.
They are probably right. But it’s worth noting that we’ve gone from “hospitals want to over-treat you” to “insurers want to under-treat you” to “life insurers want to keep you alive regardless of quality of life.” None of these are ideal. They’re just different failure modes.
The Third Map
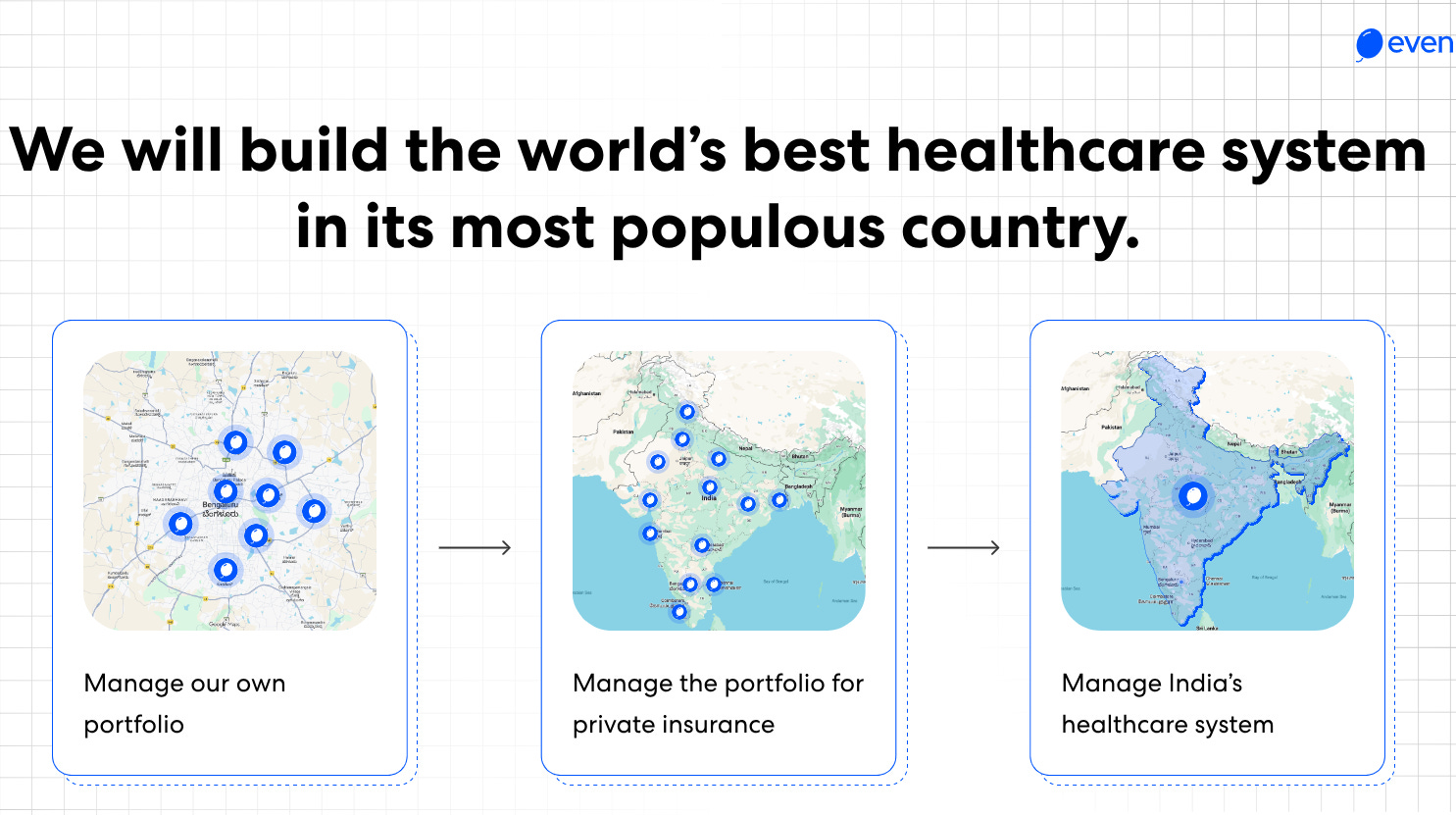
The last slide of Even’s investor deck shows three maps of India.
The first map has a cluster of blue dots around Bangalore: “Manage our own portfolio.”
The second map shows blue dots scattered across major cities: “Manage the portfolio for private insurance.”
The third map is entirely shaded blue, covering the whole subcontinent: “Manage India’s healthcare system.”
If you ask a typical Silicon Valley founder about their endgame, they’ll say something vague about “transforming” their industry. Even’s deck literally ends with “We will build the world’s best healthcare system in its most populous country.”
Most people see that slide and think it’s venture capital performance art; the kind of hyperbolic vision statement you put in a pitch deck to get Sequoia excited. But when you understand the structural forces reshaping Indian healthcare, and when you look at what the government is quietly doing, that third map stops looking like fantasy and starts looking like the only logical endpoint.
Here’s why.
Right now, the Indian government is executing a strategic retreat from healthcare delivery that it hasn’t fully articulated in public but is telegraphing through its budget allocations.
For seventy-five years, the government’s plan for healthcare was essentially: “We will be the doctor.” It turns out that being the doctor is a labor-intensive, HR-heavy, low-margin business that requires you to actually hire people and make sure the plumbing works.
The government has run the experiment of being a healthcare provider for 75 years. The PHCs remain structurally broken: 30% medical officer shortfall, 73% surgeon vacancies at Community Health Centers, facilities serving 35,000+ people against a 30,000 norm, persistent issues with medicine pilferage and staff absenteeism. These aren’t new problems; they’ve been documented for decades. You cannot fix a fundamentally broken delivery system by throwing more money at the same broken incentive structure.
So, they’re pivoting, from being a “provider” (the entity that employs doctors and owns hospitals) to being a “payer” (the entity that writes checks to others who actually deliver care).
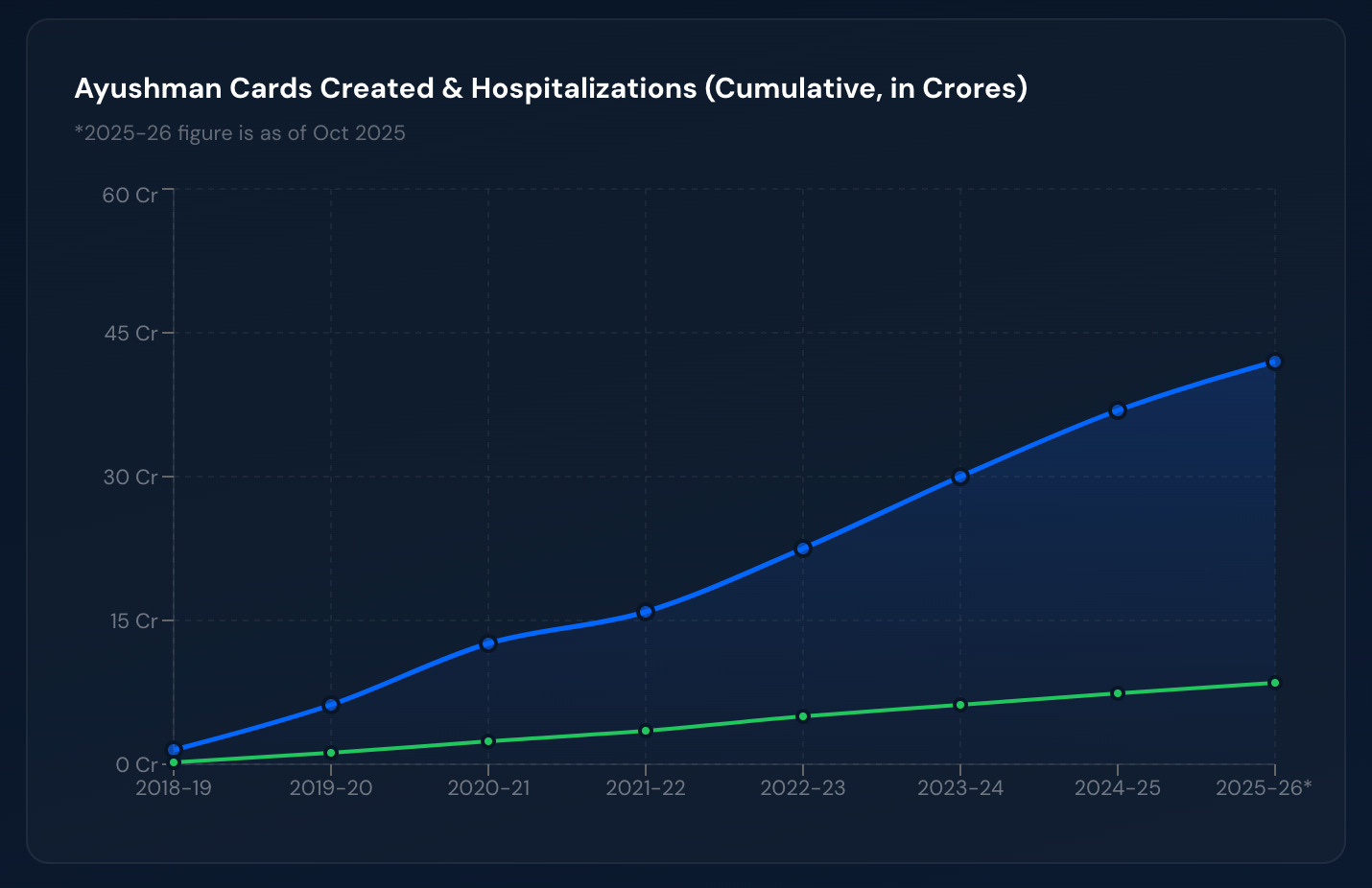
PM-JAY (Pradhan Mantri Jan Arogya Yojana), the Ayushman Bharat health insurance component launched in 2018, is the clearest signal. It now covers over 42 crore beneficiaries, nearly a third of India’s population. The government’s message is clear: “We will pay for your healthcare. We will not deliver it.”
But here’s the problem: PM-JAY is currently struggling with the same utilization issues that plague all fee-for-service insurance schemes.
The government contracts with thousands of private hospitals to deliver care under fee-for-service. Predictably, the hospitals do what fee-for-service hospitals always do: they maximize procedures. Government audits have found that a small but statistically significant percentage of claims involved unnecessary procedures, inflated billing, or outright fabricated treatments. Cataract surgeries are being performed on people who don’t have cataracts. Hysterectomies are being recommended for conditions that don’t require them.
The costs are rising significantly. PM-JAY’s funding grew 6% to ₹9,500 crore in the latest budget, now representing 9% of the ministry’s total health outlay, while quality and fraud concerns persist.
The government is learning what every insurance company eventually learns: if you pay hospitals by the procedure, hospitals will find procedures to do. You cannot control costs without controlling care delivery. But the government also knows it cannot run care delivery itself. The PHC experiment proved that.
So, the government is trapped. It needs integrated care delivery, but it cannot build or operate it. It needs someone else to own the problem.
This is the structural vacuum that Even’s “third map” is designed to fill.
In January 2026, Even raised a $20 million Series B extension, bringing Even’s total raise to $70 million was co-led by Lachy Groom and Alpha Wave, with Sharrp Ventures joining the cap table for the first time. The round was raised to expand the hospital footprint beyond Race Course Road and scale the managed-care model across Bangalore before taking it to other cities.

Could Even be your healthcare system?
The future that Even is building toward looks like this:
A state government approaches them and says, “We have 12 million Ayushman Bharat beneficiaries. We’re currently spending ₹3,800 per person per year through fee-for-service contracts with private hospitals. The fraud is rampant. The costs are rising 12% annually. The patient experience is terrible. We need something better.”
Even’s response: “Pay us ₹3,000 per person per year, fixed. We’ll take full responsibility for their healthcare.”
Here’s the exchange:
The government gets:
Fixed costs: ₹3,000 per person means a predictable annual budget of ₹36,000 crores. No more overruns.
Fraud elimination: Even isn’t billing per procedure. The incentive to fabricate treatments disappears.
Better outcomes: Even makes money by keeping people healthy, not by maximizing hospitalizations.
Political cover: The government can claim credit for improved healthcare access without actually having to run the system.
Even gets:
Massive scale: 12 million lives in a single contract, massively adding to their current total member base.
Revenue certainty: ₹36,000 crores annually, government backed. That’s the kind of revenue visibility that makes lenders very happy.
Aligned incentives: Every preventable hospitalization is the margin they capture. Prevention becomes the profit center.
Proof of universality: If they can make the model work for the Ayushman Bharat population, which is poorer and sicker than their current base, they’ve proven the model works for anyone.
Not a bad deal, for both parties.
[XIV] The Family, Again
Remember the family from the opening of this piece? The one that liquidated farmland, cashed out mutual funds, and depleted a Provident Fund to pay a ₹2,75,000 hospital bill for the mother’s cardiac emergency?
If Even’s vision plays out, if state governments shift to capitation-based integrated care contracts, here’s what changes for them:
The family is now covered under a government health scheme, managed by Even (or an Even-inspired competitor). When the mother has chest pain at 3 AM, they call a telehealth doctor who triages her in 8 minutes. If it’s serious, she’s routed to a clinic or hospital where the doctors are salaried, the incentives are aligned with outcomes, and there’s no “estimate desk” trying to maximize revenue per encounter.
If she needs a stent, she gets it. The cost is borne by the capitation contract. The family’s out-of-pocket expense is ₹0. There’s no forced liquidation of assets. No medical bankruptcy. No desperation.
And here’s the structural beauty: the system makes money by preventing that emergency in the first place. Six months earlier, when her hypertension was detected in a routine screening, the system spent ₹5,000 managing it proactively because that ₹5,000 prevented a ₹2,00,000 hospitalization.
The family doesn’t experience this as “disruption” or “innovation.” They experience it as healthcare that finally works the way it’s supposed to: you get sick, you get care, you get better, and your family doesn’t go bankrupt.
That’s the endgame on that third map.
The Ambition is the Point
When Mayank says “We will build the world’s best healthcare system in its most populous country,” he’s not engaging in founder hyperbole. He’s describing the structural inevitability he sees.
The government is not trying to run healthcare delivery. The current private market cannot align incentives. Someone has to build the integrated model at scale. And whoever builds it first, and proves it works, sets the standard that everyone else has to copy.
Even’s bet is that they can be that someone. And if they’re right, the third map isn’t grandiosity. It’s just the logical endpoint of fixing a system that’s been broken since before India’s independence.
The goal was never to build a unicorn. It was to give every Indian a fair shot at the same thing: a system that works when you need it most, that doesn’t bankrupt your family when it does, and that keeps you healthy enough that you rarely need it at all.
It was about giving every Indian a chance to get even.
Twenty-eight thousand words later, hopefully you have too.
To Debarun - thank you for stepping up to the plate, and showing us how deep an in-depth analysis can really be. To our readers: we hope you’ve enjoyed Debarun’s writing as much as we have. He’ll be back for another round.
If you want to help us coerce him into coming back for more guest pieces, pls feel free to share your appreciation for his work either in the comments below or via his Twitter/LinkedIn.
The Tigerfeathers Spotlight Series will continue this year. If you’re keen to throw your name in the hat or you have suggestions for future contributors, hit us up. Until then, keep your Tiger eyes sharp and your Tiger feathers sharp-er (or whatever).
More reading/watching/listening
The Hospital Rake by Debarun Karmakar
Report of the Health Survey and Development Committee (Vol IV)
Payvidors, Unbundled: Opportunities in Healthcare Fintech by a16z
As always, if you made it all the way here and you thought this was a good use of your time, it would mean a lot to us if you took a couple of seconds to share this post.

 | A guest post by
|
Debarun, this is truly illuminative writing. Until I hit the last bit about incentives being inverted becoming a thorn rather than a rose, it accepted human foibles in a ruthlessly analysed business model. And then transcended it.
It is also true that every system of trust built over decades and then accepted as part of the scenery becomes a target for scamming the hell out of it. Nothing is a better harvest than those who stop being a little cautious.
awesome article! Kudos and well done!!